Foundations
What is the Default Mode Network?
The brain regions that hum when you are not doing anything, the self that hums with them, and what psychedelics seem to do to the whole arrangement
1. What this article is
This is the fifth piece in the Foundations series. The four previous primers (DMT, Ayahuasca, 5-MeO-DMT, and Harmine and the MAOIs) introduced the molecules and the plant chemistry that this site spends most of its time engaged with. This one introduces a concept that none of those primers can fully avoid and that all of them, eventually, depend on: the Default Mode Network.
The DMN is, on one level, a neuroanatomical claim — a list of brain regions that show a particular pattern of coordinated activity. On another level, it has become one of the leading models for understanding the ordinary self-referential layer of consciousness: the narrative sense of being someone with a past, a future, and a continuing identity, and for why psychedelics produce the kind of experiences they produce. Both levels matter. The piece walks through them in that order.
The author note for this one is brief. Unlike the previous primers, DMN is a concept the writer encountered as a reader of the literature rather than as a participant in any practice. This essay is correspondingly third-person. The lived-experience material that justified itself in the ayahuasca primer would distort the analysis here — though where the model intersects with what experienced psychedelic participants commonly report, the connections are flagged.
2. The discovery
For most of the twentieth century, brain imaging — when it existed at all — was about catching the brain in the act of doing something. Researchers would scan a participant while the participant performed a task. The image was interpreted as "this is what the brain looks like when it's working on this problem." The rest of the time — the slow baseline state between tasks — was treated as noise, as the inactive state of a brain waiting for something to do.
In the late 1990s and early 2000s, that picture began to break.
The development of functional magnetic resonance imaging (fMRI) had made it possible to see ongoing patterns of brain activity in real time. Researchers — most prominently Marcus Raichle at Washington University in St Louis — noticed something odd. When participants were not doing tasks, when they were simply lying in the scanner letting their minds wander, certain brain regions actually became more active than they were during attention-demanding tasks. The same set of regions. Every time. Across different participants, different studies, different scanners.
This was the opposite of what the prevailing model predicted. It implied that the brain has a baseline state of activity that is not the absence of work — it is a different kind of work. Raichle and colleagues called it the "default mode" of brain function. The collection of regions that participated in it became, after a few years of nomenclature shuffling, the Default Mode Network.
What were these regions doing during the supposed baseline? Subsequent research, much of it conducted through the 2000s and 2010s, accumulated evidence that the DMN's activity correlated reliably with several specific cognitive functions:
- Self-referential thought — thinking about oneself, one's traits, one's history, one's future
- Autobiographical memory — recalling personal events, especially emotionally weighted ones
- Theory of mind — modelling what other people are thinking and feeling
- Mental simulation — imagining future scenarios, alternative pasts, hypothetical situations
- Mind-wandering — the unfocused, spontaneous thought that occupies most of human waking life when no task is demanding attention
Across all of these functions, the same broad set of regions activated together, with consistency that was hard to dismiss. The DMN was not just a coincidence of imaging methodology. Something coherent was happening in those regions, and that something was related — in some deep way — to the ordinary self-referential aspect of being a person.
3. The regions and what they do
Before naming the regions, a small piece of orientation. The DMN should not be imagined as a small glowing circuit in the brain labelled "self." It is a statistical and functional network inferred from patterns of coordinated activity across regions that fire together more reliably than chance would predict. Different papers draw its boundaries slightly differently, and some researchers divide it into subnetworks with distinct functional roles. The list below gives the standard primer-level version; the underlying anatomy is more contested at the edges than any single tidy list can convey.
The DMN is not one region but a network — several distinct cortical and subcortical areas whose activity is correlated with each other to a degree that makes them functionally one unit, at least in the relaxed-baseline state.
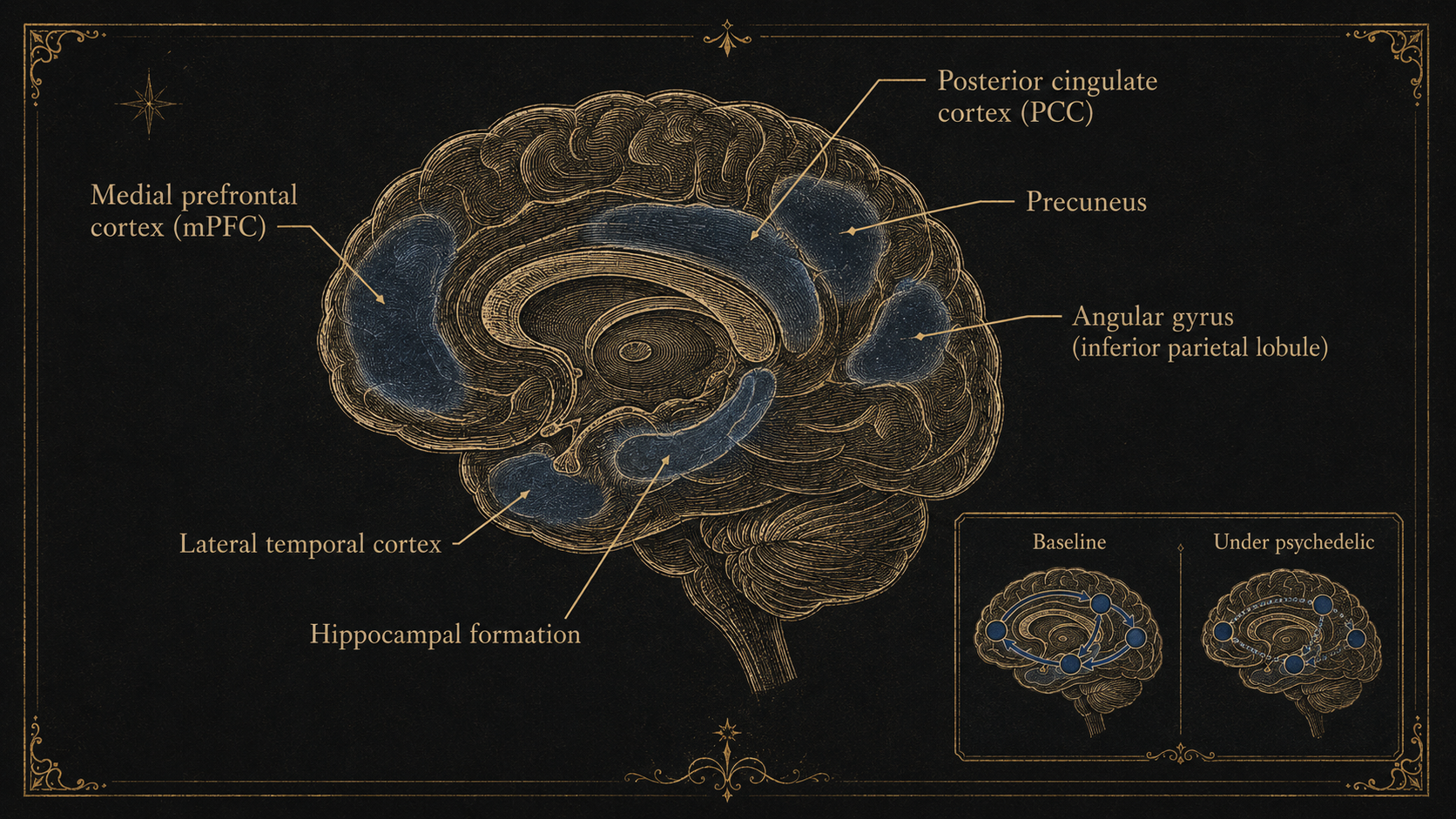
The principal nodes, in roughly descending order of how reliably they show up in DMN studies:
The medial prefrontal cortex (mPFC) — at the front of the brain on the inner wall between the two hemispheres. Strongly implicated in self-referential processing and in evaluating the personal significance of stimuli. Activity here scales with how much something matters to you specifically.
The posterior cingulate cortex (PCC) — at the back of the brain on the inner wall, behind the corpus callosum. Often described as the central hub of the DMN; it has more dense connections to other DMN nodes than any other single region. Its activity correlates particularly with mind-wandering and self-referential thought.
The precuneus — just above and slightly behind the PCC, on the inner wall. Involved in autobiographical memory, mental imagery, and the sense of being a self located in space and time.
The lateral parietal cortex / angular gyrus — on the outer surface of each hemisphere, near the temporo-parietal junction. Involved in theory of mind, in integrating information across senses, and in some aspects of self-other distinction.
The lateral temporal cortex — middle and inferior temporal regions, on the outer surface. Involved in conceptual knowledge about self and others.
The hippocampal formation — deep in the medial temporal lobe. Involved in autobiographical memory and in the construction of imagined future scenarios from past experience.
When the DMN is humming along at its baseline activity — when the regions are firing in their coordinated pattern — the felt experience is something like being a self. Thoughts about your own past, your own future, your own relationships, your own concerns, drift through awareness with the easy continuity that ordinary self-experience has. You are aware of being you. You have a name, a history, plans, opinions, an autobiography. The DMN, on one influential contemporary account, is doing much of the work of supporting that experience.
4. The ordinary self
This is the most ambitious claim associated with the DMN, and it deserves to be set out carefully because it is the claim that makes the network interesting beyond clinical neuroscience.
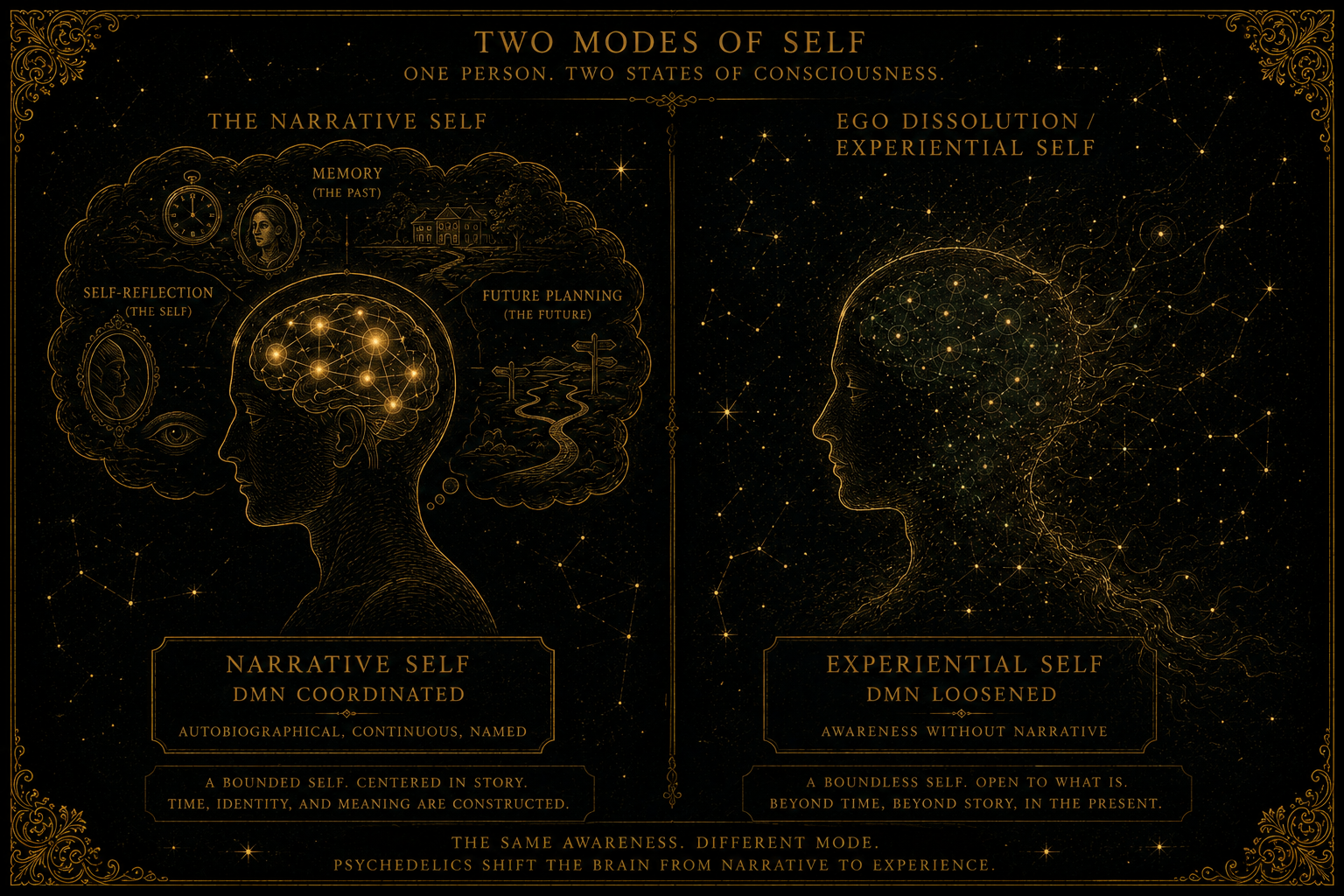
The DMN model proposes that the ordinary sense of being a continuous, narrative self — the sense most people have most of the time, that there is someone here who has experiences, makes decisions, holds memories, and faces a future — is to a considerable extent the product of the DMN's coordinated activity. The self is not located in one region of the brain. It is constructed, moment by moment, by a distributed network that integrates self-referential thought, autobiographical memory, future simulation, and social modelling into a single coherent felt experience of being a person.
This is sometimes called the narrative self or the autobiographical self, in contrast to the more minimal experiential self — the bare sense of being conscious, of there being something it is like to be you, which probably depends on broader brain activity than the DMN alone. The DMN's distinctive contribution is the narrative layer: the running internal story about who you are.
If this model is correct — and it is one influential view in cognitive neuroscience, though by no means uncontested — then several things follow that matter for the rest of this essay.
First, the narrative self is not a fixed property of being human. It is a particular configuration of brain activity, and that configuration can be disrupted, attenuated, or transformed. Different states of consciousness — meditation, sleep, anaesthesia, psychotic episodes, near-death experiences, and (most relevantly for this site) psychedelic states — show characteristic changes in DMN activity that correspond to characteristic changes in the felt sense of being a self.
Second, the considerable mental effort the DMN expends on its self-referential work has both costs and benefits. The benefits include continuity of identity, autobiographical coherence, capacity for long-term planning, and theory of mind. The costs, in the contemporary popular literature, are often described as rumination, self-criticism, anxiety about the future, and the kind of repetitive self-focused thought that characterises depression. Several clinical conditions — depression, anxiety, post-traumatic stress disorder, obsessive-compulsive disorder — are now associated with DMN hyperactivity or with abnormal DMN connectivity patterns. Treating these conditions, on one current view, involves loosening the grip of an over-active DMN.
Third — and this is where the model becomes directly relevant to ARDMT's central subject — substances that demonstrably reduce DMN activity might be expected to produce experiences in which the ordinary sense of self is loosened, attenuated, or temporarily absent. They might also be expected to have therapeutic potential in conditions where the ordinary sense of self is the problem.
This is, more or less, what the psychedelic-DMN research programme has been investigating since about 2012.
5. The psychedelic connection
In 2012, Robin Carhart-Harris and colleagues at Imperial College London published a paper in the Proceedings of the National Academy of Sciences (PNAS) reporting the results of an fMRI study of participants under the influence of psilocybin. The paper, titled "Neural correlates of the psychedelic state determined by fMRI studies with psilocybin," is widely regarded as the founding scientific document of contemporary psychedelic neuroscience.
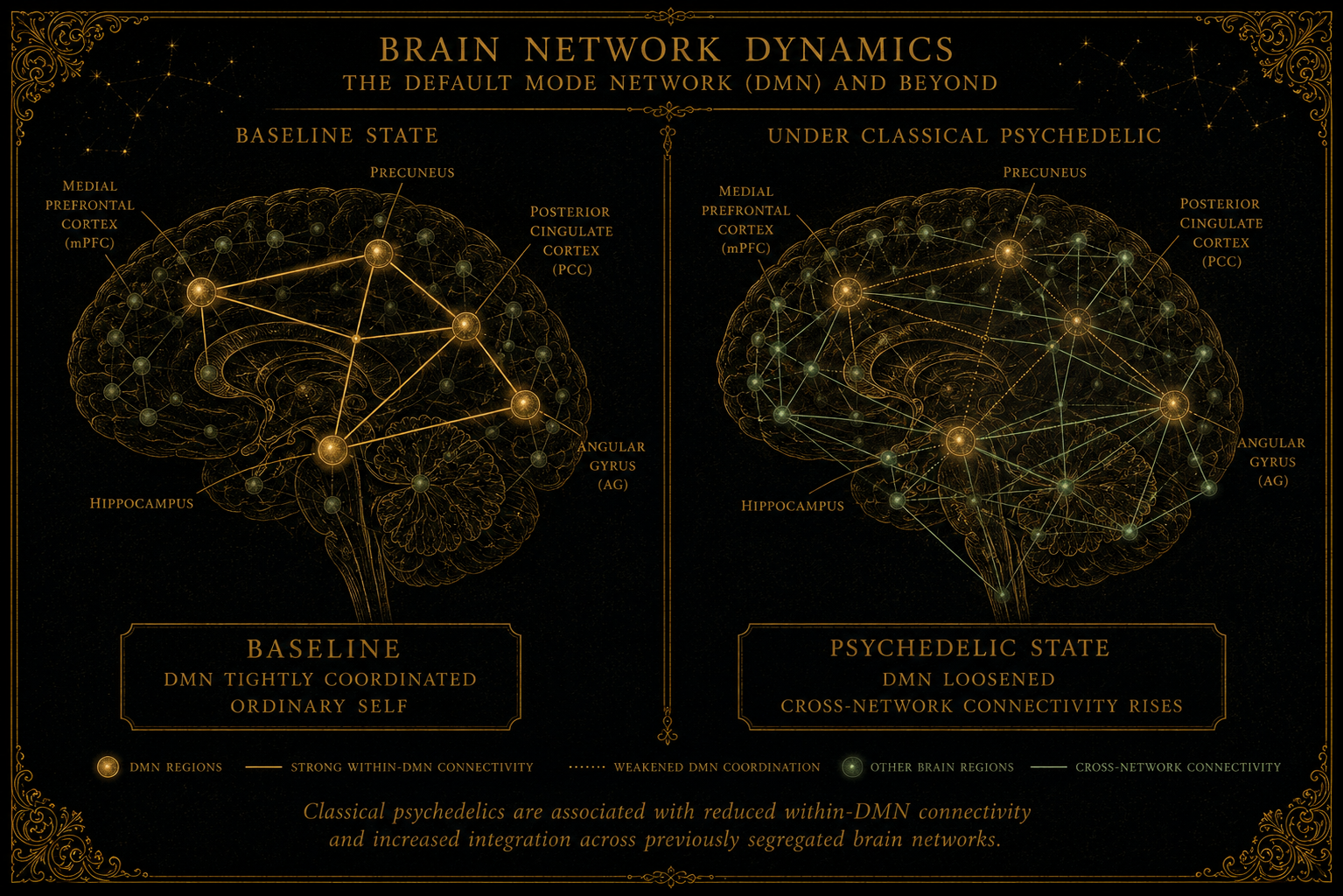
The headline finding was striking. Participants on psilocybin showed decreased activity and reduced functional connectivity in the Default Mode Network. The same regions that hum together during baseline self-referential thought were quieter and less coordinated when the participants were in the psychedelic state. The reduction was greatest at the peaks of the subjective experience and correlated with self-reports of ego dissolution.
This finding had been broadly anticipated by some — the philosophical and contemplative traditions had long described psychedelic and meditative states as involving a kind of dissolution of ordinary self — but it had never been directly demonstrated at the level of brain activity before. The DMN model and the psychedelic experience appeared, in those imaging results, to fit together.
Subsequent work, much of it from Carhart-Harris's group and from collaborating laboratories at Hopkins, Maastricht, Zurich, and elsewhere, has extended and refined the picture. Some of the most important findings include:
The effect is not unique to psilocybin. Similar DMN attenuation has been observed with LSD, ayahuasca, DMT, and (in some studies) other psychedelics. The broad finding that psychedelics alter DMN activity and connectivity has been replicated across multiple studies, although the exact pattern varies by substance, dose, method, and analysis. The pattern appears to be a general feature of the classical psychedelic state rather than a quirk of any particular compound.
The DMN doesn't just quiet — it desegregates. More refined analyses suggest that what psychedelics do is not simply turn the DMN off, but disrupt its tight internal coordination. Regions that ordinarily fire in synchrony begin to communicate more loosely. At the same time, normally segregated brain networks begin to communicate more with each other. The brain under psychedelics has been described as showing increased "global functional connectivity" alongside decreased within-network connectivity. The metaphor often used is that the brain becomes temporarily more interconnected and less hierarchical.
The disruption correlates with subjective effects. The degree of DMN attenuation in individual participants tracks with their reported intensity of ego dissolution, with the vividness of the experience, with the persistence of post-session psychological changes, and (in clinical contexts) with therapeutic outcomes. This is not just an incidental finding alongside the psychedelic state; it appears to be tracking something central to what the state actually is.
Long-term effects on DMN function follow some sessions. Several studies have reported that participants show altered DMN connectivity weeks or months after a psychedelic session, and that these alterations correlate with improvements in mood, reductions in depressive symptoms, and other clinical changes. The model that has been proposed — and is still being actively debated — is that psychedelic experiences may produce a kind of "reset" of DMN function, loosening pathological patterns and allowing healthier configurations to consolidate.
Carhart-Harris and colleagues have developed a broader theoretical framework — the entropic brain hypothesis, later refined into the REBUS (relaxed beliefs under psychedelics) model — to interpret these findings. The basic claim is that psychedelics increase the entropy or disorder of brain activity, which corresponds to a relaxation of the strong top-down predictive models the brain ordinarily uses to construct experience. Under this relaxation, ordinarily-suppressed sensory and emotional content can break through; ordinarily-rigid beliefs and self-models can soften and reconfigure. The DMN, in this framework, is the principal seat of the top-down predictive work whose relaxation defines the psychedelic state.
This framework is influential but not universally accepted. Several alternative interpretations of the same imaging data exist, and the field's confidence in any specific neurobiological story about psychedelics should be calibrated carefully. The DMN-attenuation finding has been broadly replicated, though the specific pattern depends on substance, method, and dose. The theoretical framework that interprets it is more provisional still.
6. What ego dissolution probably is
The phrase ego dissolution has become widely used in popular psychedelic discourse and is one of the more consistently reported features of higher-dose psychedelic experiences. It is also, as concepts go, slippery: people use it to mean somewhat different things, and the distinctions matter.
The clearest version of the term refers to a state in which the ordinary felt sense of being a discrete self — located in a body, with a personal history, a name, an inside and an outside — loosens, attenuates, or temporarily disappears. Participants describe variations on a theme: that the boundary between self and world becomes permeable; that the sense of being someone observing experience gives way to experience without an observer; that what is usually felt as "me thinking" comes to feel like "thinking happening, with no one in particular doing it"; that the personal historical self drops away and something more elemental remains.
Whether what remains is described as luminous, terrifying, divine, void, neutral, blissful, or some combination depends heavily on the individual, the substance, the dose, and the setting. The phenomenology varies enormously. The structural feature — the loosening of the ordinary self — is what the term "ego dissolution" is trying to point at.
On the contemporary neuroscientific picture sketched above, ego dissolution corresponds, at least partly, to the disruption of the DMN's coordinated activity. The brain regions that ordinarily integrate self-referential thought, autobiographical memory, and the felt sense of being a person quiet down and become less synchronised. The construction of the ordinary self loosens. What remains is awareness without its usual self-referential overlay.
This is a model. It is the best current model the field has. It is not the same thing as having explained the phenomenon — there are deep philosophical questions about consciousness and selfhood that no amount of brain imaging will settle, and the imaging itself is correlational rather than causal. But it is a model that has held up well across a substantial body of empirical work, and it is the model that makes most of the psychedelic-clinical-research story coherent.
A few clarifications worth registering plainly.
Ego dissolution is not the same as ego death. The latter is a more extreme phenomenology, often used to describe the experience of the personal self appearing to die during a high-dose session. Both probably involve DMN attenuation, but ego death corresponds to a more profound and longer-lasting subjective absence of self than the looser ego dissolution.
Ego dissolution is not unique to psychedelics. Deep meditation, near-death experiences, certain extreme physical states, certain spontaneous spiritual experiences, and (in pathological form) some psychotic episodes can all produce phenomenologies that look related at the level of subjective report. The DMN model is consistent with this: any state that sufficiently disrupts DMN function might produce comparable experiences, regardless of how the disruption was induced.
Ego dissolution is not inherently positive or therapeutic. Some participants find these experiences profound and beneficial. Some find them terrifying. Some find them both. The reduction of the ordinary self can be experienced as liberation or as catastrophe; the difference depends on the participant, the preparation, the context, and what surfaces when the ordinary self quiets. This variability is one of the reasons reputable psychedelic therapy emphasises preparation and integration as much as the dosing session itself.
7. What the model can and cannot explain
The DMN-psychedelics framework explains a lot. It also has real limits, and a primer is the right place to flag both.
The model accounts well for: the consistent reports of self-loosening in psychedelic states; the correlation between subjective ego dissolution and brain imaging; the general parallels between psychedelic states and other states known to involve DMN attenuation (meditation, dreaming, certain near-death experiences); the emerging therapeutic results in conditions characterised by excess self-focused processing (depression, OCD, end-of-life anxiety); and the broad finding that psychedelic effects across compounds share more features than their pharmacological differences would predict.
The model accounts less well for: the specific phenomenological differences between substances (why does DMT produce entity-encounter reports while 5-MeO-DMT produces dissolution into featureless awareness, if both reduce DMN activity?); the specific cultural and individual variability in psychedelic experiences (the same brain network change does not produce the same experience across people); the long-term changes in personality, worldview, and behaviour that psychedelics sometimes produce, which last far longer than any acute DMN change; and the philosophical question of what is actually happening during ego dissolution — what, if anything, persists when the narrative self quiets.
The model is also subject to a more general caution. fMRI is a powerful tool but a coarse one. The temporal resolution is poor (each measurement averages over several seconds), the spatial resolution is finite, and the relationship between blood flow (which is what fMRI actually measures) and neural activity is indirect. The DMN as a construct is real and well-replicated, but the specific neural mechanisms underlying its function — and underlying psychedelic effects on it — remain only partially understood.
A further consideration. The DMN model is one current framework for thinking about what psychedelics do. There are others. Some researchers emphasise the thalamocortical disinhibition that 5-HT2A activation produces. Some emphasise effects at intracellular receptors. Some emphasise the entropic-brain framework. Some emphasise neuroplasticity mechanisms that act on longer timescales than the acute experience. These frameworks are not necessarily incompatible — they may describe different levels or different timescales of the same underlying process — but the field has not yet converged on a single unified account, and the appropriate epistemic posture is to hold any one framework provisionally.
What is consistent across frameworks is that something coherent is happening when humans encounter classical psychedelics, that this something involves a recognisable disruption of ordinary cortical function, that it correlates with reports of self-loosening, and that the experiences it produces can have durable effects on mood, behaviour, and outlook. The DMN model is the current leading account of how these pieces fit together. It is probably partly right, probably partly incomplete, and probably destined to be refined or superseded by something more comprehensive over the coming decade.
8. Is there a legal dimension?
The DMN itself has no legal status. It is a brain network, not a substance. The legal questions arise only when researchers use controlled substances to study how the network behaves under altered states. In practice, that means DMN-psychedelic research is limited not by the legality of brain imaging — which is conducted routinely under standard research ethics frameworks everywhere — but by the licensing regimes governing psilocybin, DMT, LSD, ayahuasca, and related compounds. A forthcoming pillar essay on UK psychedelic policy will treat the wider research-licensing question in more detail.
9. What people often get wrong
A handful of recurring confusions about the DMN are worth addressing directly:
"The DMN is the ego." It contributes to the construction of the ordinary self-referential aspect of experience, but calling it "the ego" overstates what the model claims. The ego, if that concept is doing work at all, is a much broader functional pattern involving many brain regions and many mental processes. The DMN is one important part of the machinery, not the whole of it.
"Psychedelics work by switching the DMN off." They attenuate DMN activity and disrupt its functional connectivity. "Switching it off" implies a more complete disabling than the imaging actually shows. The DMN can be quieter, less coordinated, and less hierarchically dominant under psychedelics without being silent.
"DMN activity is the cause of depression." Some forms of depression involve DMN hyperactivity or abnormal connectivity patterns, and these patterns correlate with the kind of repetitive negative self-focused thought that characterises the condition. But correlation is not causation, and depression is a heterogeneous condition with many contributing factors. "The DMN causes depression" is a popular simplification of a more complicated picture.
"Meditators have permanently reduced DMN activity." Some long-term meditators show altered DMN patterns, but the relationship is more nuanced than simple reduction. Different meditation practices target different aspects of cognition, and the resulting DMN changes vary accordingly. The popular framing of meditation as "permanently quieting the DMN" oversimplifies the research.
"Ego death is the goal of psychedelic therapy." It is one experience that can occur during psychedelic therapy. It is not consistently associated with better therapeutic outcomes. Plenty of participants benefit from psychedelic-assisted treatment without experiencing ego death; some who experience it do not benefit. The goal of clinical psychedelic therapy is therapeutic improvement, which may or may not involve ego-dissolution experiences along the way.
"The DMN model proves consciousness is brain-based." It is consistent with the brain-based view of consciousness, but consistent-with is not the same as proves. There remain deep philosophical questions about why brain activity is accompanied by subjective experience at all — the hard problem of consciousness — that the DMN model does not address and probably cannot resolve.
10. What we still don't know
The genuinely open questions in DMN research, briefly:
How the DMN is constructed at the cellular level — what specific neurons, in what specific patterns, produce the coordinated network-level activity that fMRI detects. Most current understanding is at the network level rather than at the cellular level.
Whether the DMN as currently characterised is one network or several functionally distinct subnetworks whose activity happens to correlate. Some recent work suggests the latter; the field has not converged.
How much of what the DMN does is universal across humans versus shaped by language, culture, autobiographical particulars, and developmental history. There is some evidence of cross-cultural variation in DMN function that has not been fully characterised.
How the DMN develops across the lifespan — in infancy, through childhood, in adolescence, into old age — and how individual variability in DMN function relates to variability in personality, mood, cognitive style, and vulnerability to psychiatric illness.
Whether the entropic-brain and REBUS models will turn out to be the right interpretive framework for the DMN-psychedelics data, or whether something else is needed.
What the relationship is between DMN function and consciousness in the deeper philosophical sense — between the network activity science can measure and the felt experience of being a self that the network appears to be associated with.
These are not minor technicalities. They are why DMN research remains genuinely live as a scientific field rather than a closed one.