Understanding
What is DMT?
An orientation to the molecule behind ayahuasca, smoked DMT, and one of the strangest open questions in human pharmacology
1. What this article is
This article is the front door.
It assumes nothing. You may have come here because you read Michael Pollan, or because a colleague mentioned ayahuasca over dinner, or because a friend went to a retreat and came back changed, or because a news piece about psilocybin therapy made you wonder what else there was. It walks through what DMT is, where it shows up in the world, what it appears to do to people, what science currently understands about how it works, how the law treats it, and what is still being argued about.
It is not a guide to using DMT — and would not be useful as one even if I tried. The relationship between psychedelic compounds and the human nervous system is more complex than any article can responsibly summarise into instructions. What follows is map-making, not prescription.
By the end you should be able to read any Field Note on this site, or any deeper essay, without bouncing off the vocabulary.
2. The molecule
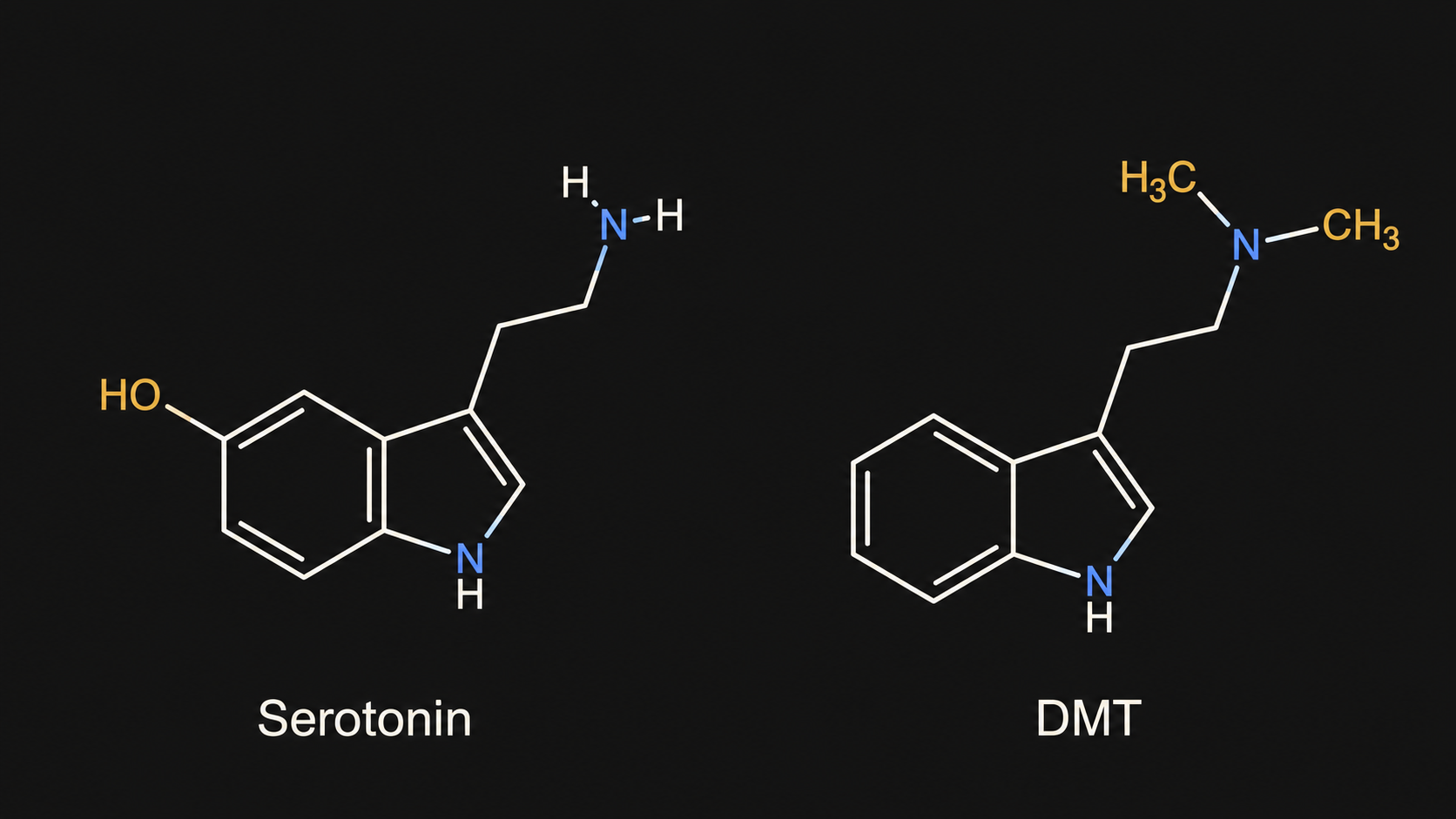
DMT stands for N,N-dimethyltryptamine. The name describes what the molecule is: a tryptamine (a small family of compounds built around a particular ring structure) with two methyl groups attached at the nitrogen atom. It is chemically very simple. If you took serotonin — the neurotransmitter most people have heard of from antidepressant adverts — and made two small modifications to it, you would have DMT.
Of the major psychedelics, DMT is among the most chemically minimal. The molecule weighs less than half what LSD does. It is structurally close to compounds the human body produces routinely. And — this is where things become genuinely strange — small amounts of DMT itself have been detected in human blood, urine, and cerebrospinal fluid for over fifty years.
Whether the body actively makes DMT in functionally meaningful amounts, and whether the trace levels detected mean anything physiological, is one of the most contested questions in neuropharmacology. There is a longer essay on this site dedicated to that question alone — Endogenous DMT in humans: a critical review of the state of the evidence — and it is not the kind of question that lends itself to a sentence-long answer. For the purposes of this primer, the headline points are:
- DMT is structurally simple, and structurally close to serotonin
- It is found, in trace amounts, in the human body
- It is found, in much larger amounts, in many plants and at least one animal (the Sonoran Desert toad — though that's a closely related molecule, 5-MeO-DMT, which we'll come to)
- Whether the body's own DMT does anything meaningful is open
The long-form argument on this is here: Endogenous DMT in Humans: A Critical Review of the State of the Evidence.
3. The forms DMT takes in the world
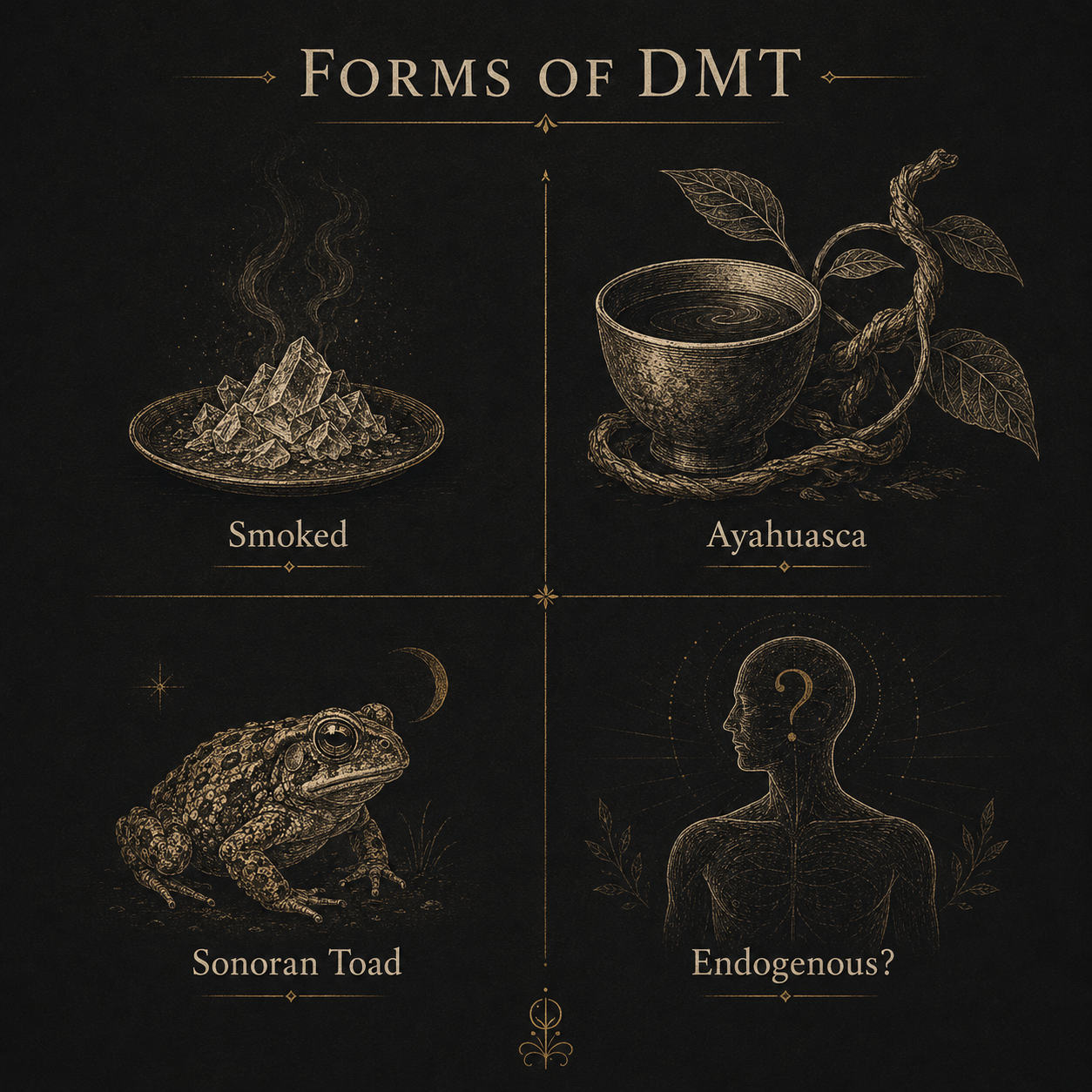
This is where most people get confused, and the confusion is worth clearing up before going further. The word "DMT" gets used to refer to several different things, and they produce different experiences.
Smoked or vaporised N,N-DMT. This is what people usually mean when they say "DMT" with the kind of breathless reverence that has made its way into podcast culture. A crystalline extract — typically obtained from plants like Mimosa hostilis or Acacia species, though it can also be synthesised — is heated and inhaled. The effects come on within seconds. They peak within two or three minutes. They are over within fifteen. Reports of the experience are intense and often described in language that sounds religious. We'll come to this in the next section.
Ayahuasca. A brew, originating in the upper Amazon, in which DMT is taken orally. There is a wrinkle: DMT taken by mouth is, by itself, broken down in the gut by an enzyme called monoamine oxidase before it can reach the bloodstream. Ayahuasca solves this problem by combining a DMT-containing plant (usually Psychotria viridis) with a second plant — typically the vine Banisteriopsis caapi — which contains compounds that temporarily disable that enzyme. The DMT then survives digestion and produces an experience lasting four to six hours.
How the indigenous peoples of the upper Amazon discovered this combination — without any of the analytical chemistry that explains it now — is one of the genuinely unanswered questions in the history of pharmacology. The traditional answer given by ayahuasca practitioners is that the plants themselves communicated the recipe. Western scientific accounts struggle to do much better.
5-MeO-DMT. Strictly a different molecule — N,N-dimethyltryptamine with a methoxy group attached at the 5-position of the ring — but pharmacologically close enough that people often lump it together with DMT. It is found in a different set of plants and, famously, in the venom of the Sonoran Desert toad (Incilius alvarius, formerly Bufo alvarius). The toad does not produce 5-MeO-DMT for human use; it produces it as a defensive secretion. People have, nonetheless, found ways to collect, dry, and smoke the venom.
5-MeO-DMT produces a profoundly different experience from N,N-DMT — less visual, more dissolving — and is currently the molecule in the most advanced stages of clinical development for depression. Its own primer is forthcoming on this site.
Endogenous DMT. As mentioned: trace amounts of DMT have been detected in human biological fluids for half a century. Whether the body is producing it deliberately, for some functional purpose, or whether it is a low-level by-product of broader amine metabolism, is unresolved. The popular claim that endogenous DMT explains dreams, near-death experiences, and the moment of dying is much stronger than the evidence supports — but the underlying question (does it have any biological role at all?) remains genuinely open.
Going deeper on the 5-MeO-DMT distinction specifically: What is 5-MeO-DMT? (forthcoming).
4. What it does
I'll keep this section deliberately brief and unsensational, because the literature on subjective effects is voluminous and the temptation to indulge it is strong.
DMT, in its smoked form, produces what is widely described as one of the most intense altered states it is possible for a chemical to induce. People report a complete dissolution of the ordinary sense of self; vivid, often geometric, visual phenomena; and — characteristically — an experience that takes the form of contact with entities, environments, or intelligences described by participants as "more real than real." Some find this revelatory. Others find it terrifying. A substantial fraction find it both, sometimes within the same fifteen-minute experience.
The afterglow is usually mild and the cognitive sequelae minimal — unusually so for a substance this powerful. People typically return to ordinary consciousness within twenty minutes, often able to drive, talk, work, or otherwise resume daily life. This rapid offset is part of why DMT is of interest as a clinical tool: unlike psilocybin or LSD, which require all-day treatment sessions, a DMT intervention could in principle fit inside a clinical hour.
Taken orally as ayahuasca, the experience is longer, slower, more thematic, and very often involves nausea — the brew has the gut as well as the brain to contend with. It is the form most commonly used in ceremonial and therapeutic contexts, where the duration is part of the point: longer experiences allow more material to surface and be worked through.
A few cautions are worth registering.
First, what people report about a drug experience is shaped, often heavily, by what they expect to report, by what cultural categories are available to describe it, and by the context in which the substance is taken. This is sometimes called "set and setting" and matters enormously. A DMT experience in an indigenous ceremonial context is reported differently from a DMT experience in a friend's flat at 2am, even when the dose and the molecule are identical.
Second, the language psychonauts have developed for DMT — "entities," "hyperspace," "machine elves" — is interpretive rather than descriptive. It is what some people have settled on as a way of describing experiences that resist ordinary vocabulary. It is not what science thinks the experience is. Treating those terms as literal claims about what DMT reveals takes them further than they were ever meant to go.
Third, DMT is not benign for everyone. People with certain psychiatric histories — particularly schizophrenia or bipolar disorder — can come to real and durable harm. People taking certain medications, especially SSRIs and MAO inhibitors, face genuine pharmacological risks. The vivid, brief, "reset-like" experience that smoked DMT can offer should not be confused with safety. Most psychedelic risk is statistical: rare in any individual, real across a population.
5. How it works in the brain
Here we leave anecdote and enter receptor pharmacology.
The brain is full of receptors — proteins on the surface of nerve cells that respond to specific chemical signals. Different drugs work by binding to different receptors, in different ways, in different parts of the brain.
Psychedelics — DMT, psilocybin, LSD, mescaline, and others — share a primary target: a receptor in the serotonin system called the 5-HT2A receptor. They are not the only compounds that bind here, but they bind in a particular way that activates the receptor with a pattern of effects that other compounds don't reproduce. Block the 5-HT2A receptor pharmacologically (with a drug called ketanserin, for instance), and the psychedelic effect almost entirely disappears. This is one of the cleanest findings in psychedelic neuroscience.
DMT binds to 5-HT2A. So far, so standard. But DMT also binds to several other targets, including — interestingly — a peculiar receptor called the sigma-1 receptor, which is found inside cells rather than on their surfaces. The role of the sigma-1 receptor in DMT's effects is debated; the leading view is that it contributes to long-term effects on neurons (growth, stress protection) rather than to the acute psychedelic experience itself. There is a forthcoming primer on the sigma-1 receptor on this site for readers who want to go deeper into this strand.
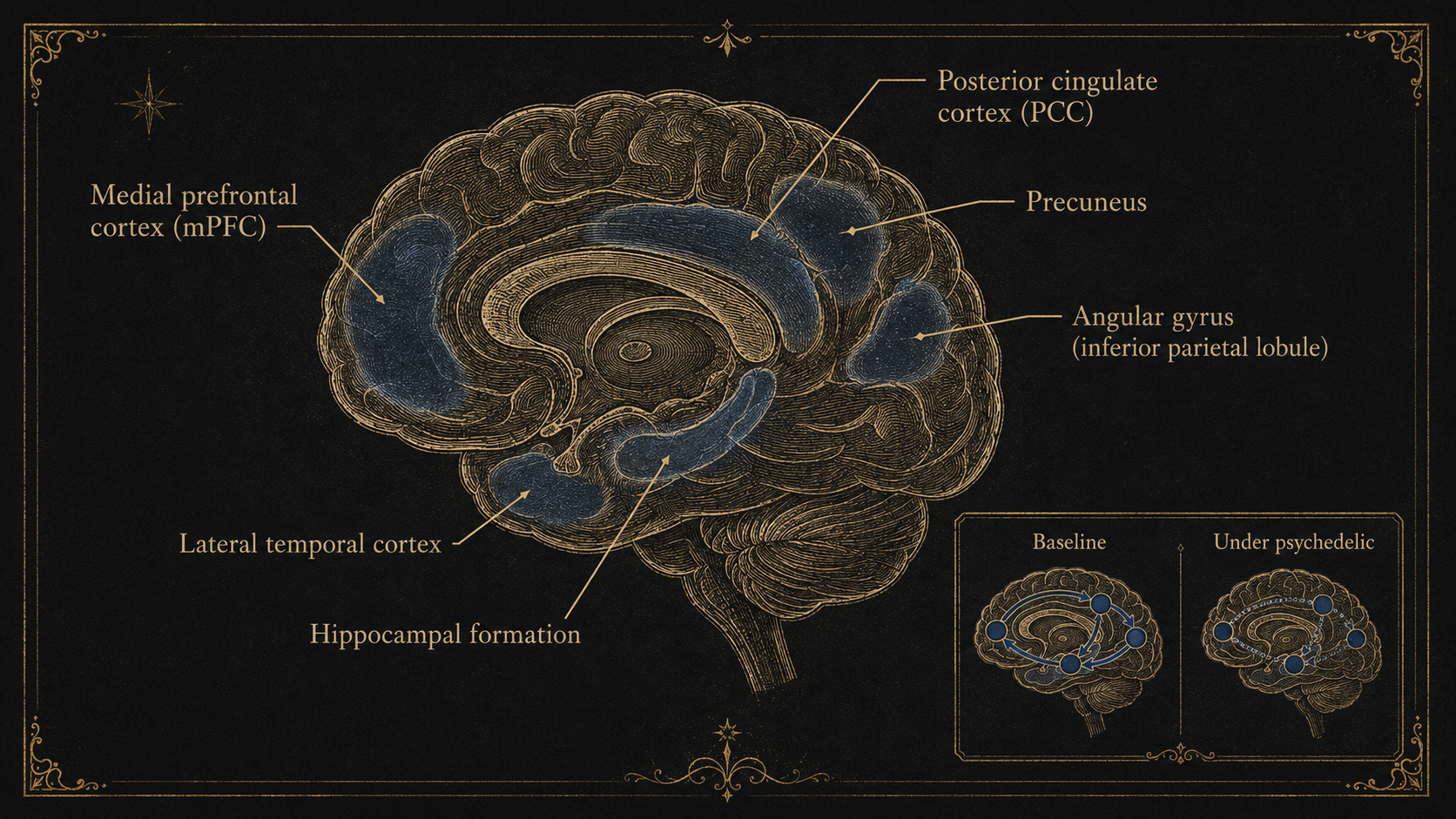
What does activating 5-HT2A actually do at the scale of the whole brain? The most current scientific answer involves a concept called the default mode network — a set of interconnected brain regions that, when humans aren't doing anything in particular, hum along together in a coordinated rhythm. The default mode network seems to underpin the ordinary sense of being a self located in a body with a history and a name. Psychedelics, particularly DMT, appear to disrupt the activity of this network. This is currently the leading neurobiological candidate for what people are experiencing when they describe "ego dissolution" on these compounds.
(A primer on the default mode network is forthcoming, for readers who want to follow this strand specifically.)
The picture is not complete. There is recent and active research into how DMT acts at receptors inside cells rather than only on their surface — work that suggests psychedelics might be doing more than the 5-HT2A story alone captures. The receptor model we currently rely on is the best available, but it is not closed.
Going deeper on the brain-network model: What is the Default Mode Network? (forthcoming).
6. The cultural story
DMT in its plant forms has a long human history — much longer than the modern scientific story.
Ayahuasca has been used for centuries across the upper Amazon for healing, divination, and ritual. The exact age of the practice is debated; some scholars argue for several thousand years, others for centuries rather than millennia. What is not debated is that ayahuasca is central to a number of indigenous Amazonian cosmologies and to several religious movements — Santo Daime, União do Vegetal, the Barquinha — that have grown up around it in the twentieth century. Other DMT-containing plants have an even older archaeological record: Anadenanthera seeds used as ceremonial snuffs have been recovered from sites in northern Chile dated to at least 2,000 BCE.
The Western scientific story is much more recent. DMT was first synthesised in 1931 by a Canadian chemist, Richard Manske, who made it as a curiosity and had no idea what it would do. The molecule sat on the shelf, pharmacologically unexamined, for twenty-five years.
In 1956 the Hungarian chemist Stephen Szára, frustrated at being unable to obtain mescaline from behind the Iron Curtain, prepared DMT himself and injected it into himself. His notes, published the following year in Experientia, are among the founding documents of modern psychedelic science. Szára described an experience that lasted under an hour, included vivid visual phenomena and altered emotional states, and resolved cleanly without after-effects. He went on to study the compound in clinical populations through the late 1950s.
Through the 1960s and 1970s, DMT became part of a much broader interest in psychedelic compounds. The transmethylation hypothesis of schizophrenia — the idea that the disorder might be caused by the body accidentally producing hallucinogenic methylated metabolites — drove a substantial empirical programme of detecting DMT in patient fluids. The hypothesis has now largely faded, for reasons covered in the Endogenous DMT review, but it generated decades of useful chemistry and analytical method along the way.
When psychedelics were criminalised across most of the Western world in the late 1960s, formal DMT research more or less stopped. Between roughly 1970 and the early 2000s, DMT became part of an underground rather than a scientific story. The molecule's modern reputation was shaped less by laboratories than by writers — Terence McKenna in particular — and later by the publication of Rick Strassman's 1994 clinical study on volunteers at the University of New Mexico, written up in his 2001 book DMT: The Spirit Molecule. Strassman's framing of DMT as a uniquely "spiritual" compound has been influential, contested, and is responsible — for better and worse — for much of the language ordinary readers encounter when they first come across the subject.
7. The modern research renaissance
Since roughly the early 2000s, scientific study of psychedelics has been re-opening. Slowly at first; then less slowly.
Several universities now have established research programmes investigating psychedelics for psychiatric and neurological conditions: Johns Hopkins in the United States, Imperial College London and University College London in the UK, Maastricht in the Netherlands, Zurich in Switzerland. The University of Exeter, relevantly to this site, runs the UK's first dedicated master's degree in psychedelic studies.
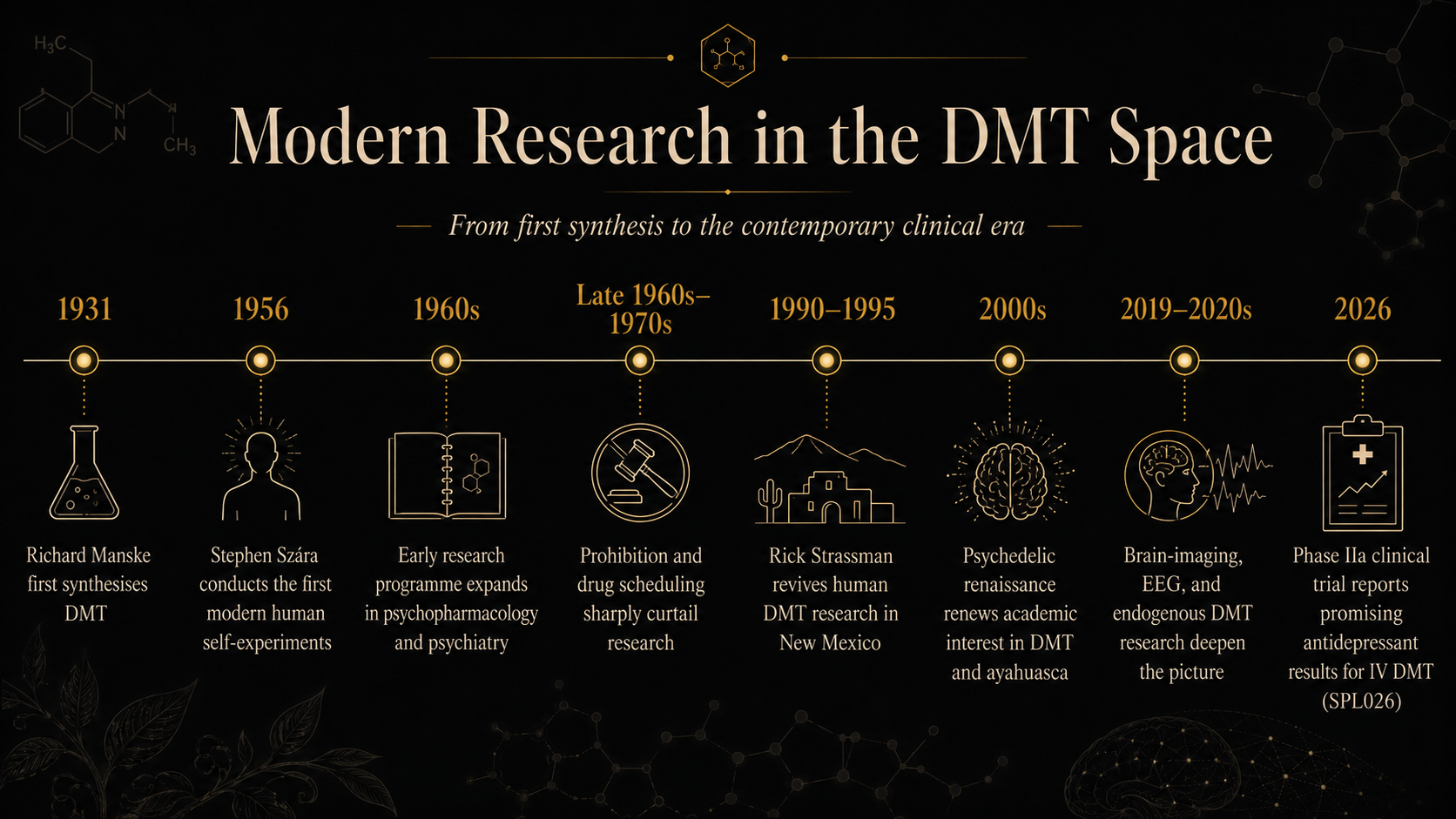
DMT specifically is the focus of several active clinical trials. The challenge that smoked DMT poses for medicine — the experience is too brief, too uncontrollable, too dependent on inhalation technique — has prompted the development of more clinically tractable delivery systems: intravenous infusions, intranasal sprays, controlled-release formulations. Imperial College's DMTx programme has been working on extended IV infusion protocols that allow the experience to be prolonged and titrated for therapy. Beckley Psytech's BPL-003 — strictly a 5-MeO-DMT formulation rather than N,N-DMT, but in the same family — has progressed through encouraging Phase 2 results for treatment-resistant depression, including, notably, in patients who remain on their existing SSRI medication.
What is being measured varies by trial: reductions in depression scores, anxiety scores, addictive behaviour, end-of-life distress. The early results are encouraging but provisional. Psychedelic clinical trials face real methodological challenges — blinding is famously difficult when the substance has unmistakable effects on the participant — and a degree of caution about the headline claims is well-placed. We track the active trials in detail in our Field Notes section, with one post per significant publication.
The political-economic question — whether psychedelic compounds will end up routinely available as licensed medicines within the next decade — is currently more open than it was eighteen months ago. The FDA's rejection of MDMA-assisted therapy in 2024 cooled expectations across the field. DMT and 5-MeO-DMT trials have continued nonetheless, and the underlying signal in the data remains interesting.
8. Is it legal?
In the United Kingdom, DMT is a Class A controlled drug under the Misuse of Drugs Act 1971, and sits in Schedule 1 of the Misuse of Drugs Regulations 2001 — the most restrictive category, formally reserved for substances with no recognised medical use.
Possession is punishable by up to seven years' imprisonment and an unlimited fine. Supply or production carries a maximum of life imprisonment. Ayahuasca, as a preparation containing DMT, is treated as DMT for the purposes of the law, even though neither the brew nor either of its constituent plants is itself a controlled substance: a 2014 Court of Appeal decision (R v Aziz) confirmed that a DMT-containing preparation is itself a Class A drug regardless of botanical origin.
There are narrow exceptions for licensed research and for limited industrial uses, granted under Home Office licence. This is how the clinical trials currently underway are legally possible. There are no exceptions for personal, religious, or ceremonial use, although prosecutions for low-level ceremonial possession have been rare. The legal landscape in the UK has not meaningfully shifted in over fifty years, though pressure is building from the research and clinical communities for reform — including a 2023 parliamentary inquiry by the All-Party Parliamentary Group on Drug Policy Reform.
Outside the UK, the picture varies. The United States classifies DMT under Schedule I federally, with religious-use exemptions granted to two ayahuasca-using churches (the União do Vegetal and Santo Daime) following Supreme Court litigation. Brazil and Peru, where ayahuasca is part of long-standing indigenous and religious practice, treat the brew differently from the molecule, allowing ceremonial use under defined conditions. The Netherlands has historically tolerated ayahuasca use within registered religious contexts. Each jurisdiction handles the question its own way; there is no international consensus.
A pillar essay on UK psychedelic law specifically, covering Schedule 1 status, the consequences for research, and the available avenues for reform, is in preparation.
9. What people often get wrong
A primer is also the right place to flag the assumptions readers may have arrived with that the literature does not support. None of these is a fringe error — all of them recur in popular writing, podcast culture, and conversation around the subject.
"DMT is the dream chemical." There is no good evidence for this. The claim originates principally with Rick Strassman's 2001 book and has not been replicated or confirmed in the twenty-five years since. Endogenous DMT may have some biological role — the longer essay examines the evidence in detail — but the specific dream-chemical claim is speculation, not finding.
"Ayahuasca is just oral DMT." No. Ayahuasca is a pharmacological system — DMT plus monoamine oxidase inhibitors, sometimes plus additional admixture plants — embedded in cultural and ritual contexts that materially shape the experience. Reducing it to "DMT in a cup" misses both the pharmacology and the practice.
"5-MeO-DMT and N,N-DMT are basically the same." They are not. Same chemical family, different molecules, different receptor preferences, profoundly different subjective effects. Treating them as interchangeable is one of the most common errors in popular psychedelic writing.
"Iboga contains DMT." It does not. Iboga and DMT share a distant biosynthetic ancestor in tryptophan metabolism, but the iboga-type alkaloids are structurally complex pentacyclic compounds, not tryptamines. The iboga experience is the ibogaine experience, not a DMT experience.
"Natural means safe." Plant-derived does not mean low-risk. Ayahuasca interacts with several common medications — SSRIs in particular — in ways that can be dangerous. Ibogaine has caused deaths through cardiac complications. The natural origin of a compound is a fact about its history, not its safety profile.
"DMT is addictive." There is no clinical or pharmacological evidence of physical or behavioural addiction to DMT. People who take it repeatedly often describe diminishing returns rather than craving. This does not mean the substance is risk-free, but the addiction frame is misapplied.
"Spiritual reports prove what was experienced was real." People genuinely report experiences they describe in spiritual or metaphysical terms, and those reports are real reports — the experiences happened. Whether the reports are evidence for the external reality of what was perceived is a separate question. Conflating "this happened to me" with "this proves the entity I encountered exists" is an epistemic move that requires considerably more support than the reports themselves provide.
10. What we still don't know
A primer is not the place to settle questions; it is the place to flag which ones are still open. The honest list, briefly:
Whether the human body makes DMT in functionally meaningful amounts, and if so, for what purpose. (Covered in detail in the Endogenous DMT essay.)
What, exactly, the experience of intense DMT states is, beyond the descriptions participants give of it — and whether the consistent entity reports across cultures reflect anything beyond the brain's tendency to populate ambiguous sensory input with social presence.
Whether DMT will prove durably useful as a psychiatric medicine, or whether early trial enthusiasm will moderate as more data arrive and follow-up periods lengthen.
How much of what we know about DMT pharmacology in rats — which is most of what we know — translates faithfully to human beings.
Whether the receptor models we currently rely on (5-HT2A, sigma-1, others) capture what is actually happening when DMT meets a human nervous system, or whether there are aspects of its action we haven't yet identified. Recent work on intracellular receptor activity suggests the picture is genuinely not closed.
What the relationship is, in any deep sense, between the chemistry of DMT and the cultural and ceremonial frameworks that humans have built around it for thousands of years.
These are not gaps to be papered over. They are why the field is worth taking seriously.