Foundations
Harmine and the MAOIs
The plants that make ayahuasca possible, the enzymes they switch off, and a research strand that may be on the verge of becoming a medicine of its own.
1. What this article is
This is the fourth in the Foundations series, and the most chemically focused of the four. The first three primers (What is DMT?, What is Ayahuasca?, and What is 5-MeO-DMT?) covered substances most readers had heard of even before they arrived. This one introduces a class of compounds — the β-carbolines, with harmine as the principal representative — that most readers will not have heard of, but that they cannot understand the ayahuasca story without.
The piece walks through what the β-carbolines are, where they come from, what they do, the enzyme system they act on, why that enzyme system matters far beyond ayahuasca, the safety implications of inhibiting it, and the recent emergence of harmine as a research compound on its own merits. It assumes no biochemistry background and builds the necessary detail as it goes.
A small note on what this article is not. It is not a guide to combining MAO inhibitors with anything; the SSRI–MAOI–serotonergic-drug interaction risk is serious and real and outside the scope of a primer to discuss in operational detail. The pharmacology is here because the pharmacology matters; the application is not.
2. What β-carbolines are
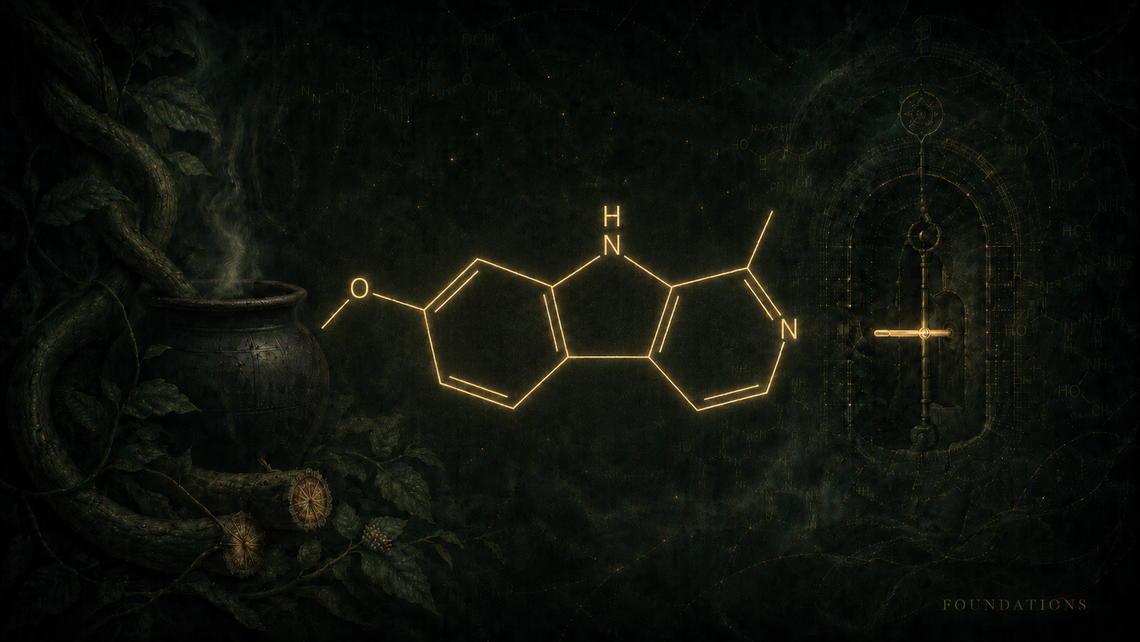
β-carbolines are a class of organic compounds defined by a particular three-ring molecular structure: an indole fused to a pyridine ring, with the nitrogen atom positioned in a way that gives the family its name. The family is large — chemists have characterised dozens of natural and synthetic β-carbolines — and its members are widespread in nature, appearing in plants, fungi, and animals.
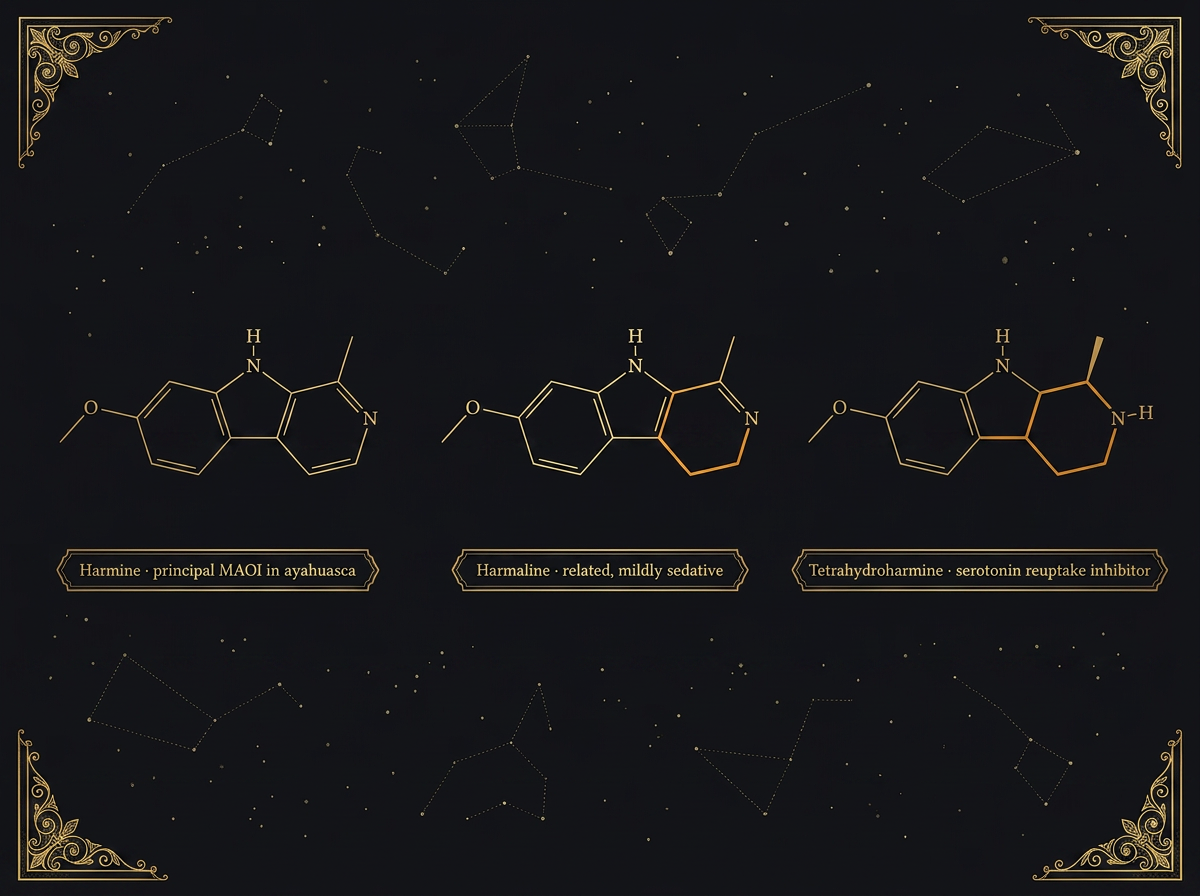
The three β-carbolines that matter most for ayahuasca, in roughly descending order of typical concentration in the brew, are:
- Harmine — the most abundant β-carboline in Banisteriopsis caapi and the principal active inhibitor of monoamine oxidase in the brew
- Harmaline — closely related to harmine, slightly more sedating, mildly psychoactive at higher doses
- Tetrahydroharmine (THH) — structurally similar but with different activity; an inhibitor of serotonin reuptake rather than (primarily) MAO
These three together account for nearly all of the pharmacologically relevant β-carboline content of a typical ayahuasca brew. Other β-carbolines exist in much smaller quantities and probably contribute marginally if at all.
The β-carbolines occur in many natural sources beyond B. caapi — the most familiar being the seeds of Peganum harmala (Syrian rue), an arid-region plant native to the Mediterranean, Middle East, and parts of central Asia. Syrian rue contains harmine and harmaline in concentrations even higher than B. caapi, and has its own ancient ceremonial and medicinal history in those regions. Whether Syrian rue has been used historically as an MAOI to make oral DMT-containing plants psychoactive — analogous to ayahuasca's vine — is a contested ethnobotanical question. The pharmacological capacity is unambiguously there; whether it was deliberately exploited in any specific historical tradition is harder to establish.
3. The enzyme they act on
To understand what harmine and its relatives do in the body, we need to spend a moment on the enzyme they switch off — because the pharmacology only makes sense once that enzyme has been properly introduced.
Monoamine oxidase (MAO) is a family of enzymes whose role in the body is to break down a particular class of small molecules called monoamines. The category includes some compounds the body needs to dispose of routinely (dietary amines from food), and several compounds the body uses as neurotransmitters or hormones (serotonin, dopamine, noradrenaline, adrenaline, melatonin) once they have done their work. MAO exists in two forms: MAO-A and MAO-B, each with overlapping but distinct substrate preferences, and each present in different proportions across different tissues.
MAO-A preferentially breaks down serotonin, noradrenaline, and (importantly for ayahuasca) tryptamines including DMT. MAO-B preferentially handles dopamine, phenethylamine, and some other monoamines. Both enzymes exist throughout the body but the gut and liver are particularly rich in them — which is part of why oral DMT-containing plants are pharmacologically inert without an inhibitor. The MAO in the gut wall and the liver's first-pass metabolism intercepts any tryptamine before it reaches the systemic circulation.
Inhibiting MAO — temporarily switching the enzyme off — therefore has two principal effects. First, it allows substrate compounds (including DMT) to survive what would otherwise be rapid destruction. Second, it raises the body's baseline levels of the neurotransmitters that MAO normally clears. Both effects matter; the second is the source of most of the clinically significant interactions and risks of MAO inhibition.
This is not a niche pharmacology. MAO inhibitors were among the first effective antidepressant medications, introduced in the late 1950s before SSRIs existed; some are still in clinical use today (phenelzine, tranylcypromine, moclobemide, selegiline) for specific psychiatric and neurological indications. The MAO inhibitors of ayahuasca and the MAO inhibitors of contemporary psychiatry are pharmacologically siblings, even if their cultural contexts could hardly be more different.
4. Two kinds of MAO inhibition
A distinction worth understanding clearly, because it bears on safety questions later in the essay: not all MAO inhibitors are the same kind of MAO inhibitor.
Irreversible MAOIs — including the older antidepressants phenelzine and tranylcypromine — bind to MAO in a way that permanently disables the enzyme molecule they have bound. The body recovers its MAO function only by synthesising fresh enzyme over the following weeks. Effects therefore last long after the drug itself has cleared, and pharmacological interactions persist for two to four weeks after the last dose. Patients on irreversible MAOIs require strict dietary restrictions (avoiding aged cheeses, cured meats, fermented products, and other tyramine-containing foods) and equally strict drug-combination caution. These were once first-line antidepressants and are now reserved for treatment-resistant cases.
Reversible MAOIs — including harmine and the other β-carbolines in ayahuasca — bind to MAO in a way that can be displaced. The enzyme molecule recovers normal function once the inhibitor has cleared. Effects therefore correspond fairly closely to the drug's pharmacokinetic profile: hours rather than weeks. The dietary restrictions associated with irreversible MAOIs apply only loosely to ayahuasca; serious tyramine-induced hypertensive crises are uncommon with reversible inhibitors, although some caution about high-tyramine foods in the 24 hours before and after a ceremony remains sensible.
This distinction matters for ayahuasca specifically because the safety profile of the brew is meaningfully better than the safety profile of older irreversible MAOIs would suggest. Indigenous ceremonial practice does not require the weeks-long dietary regimen that 1960s antidepressant medicine did. In that respect, the brew is pharmacologically more forgiving than the first generation of pharmaceutical MAOIs.
What it does not change, however, is the risk of combining ayahuasca with other serotonergic drugs — which §6 will return to.
5. The DMT–harmine interaction
This is the headline pharmacology, and the reason ayahuasca exists as a brew at all.
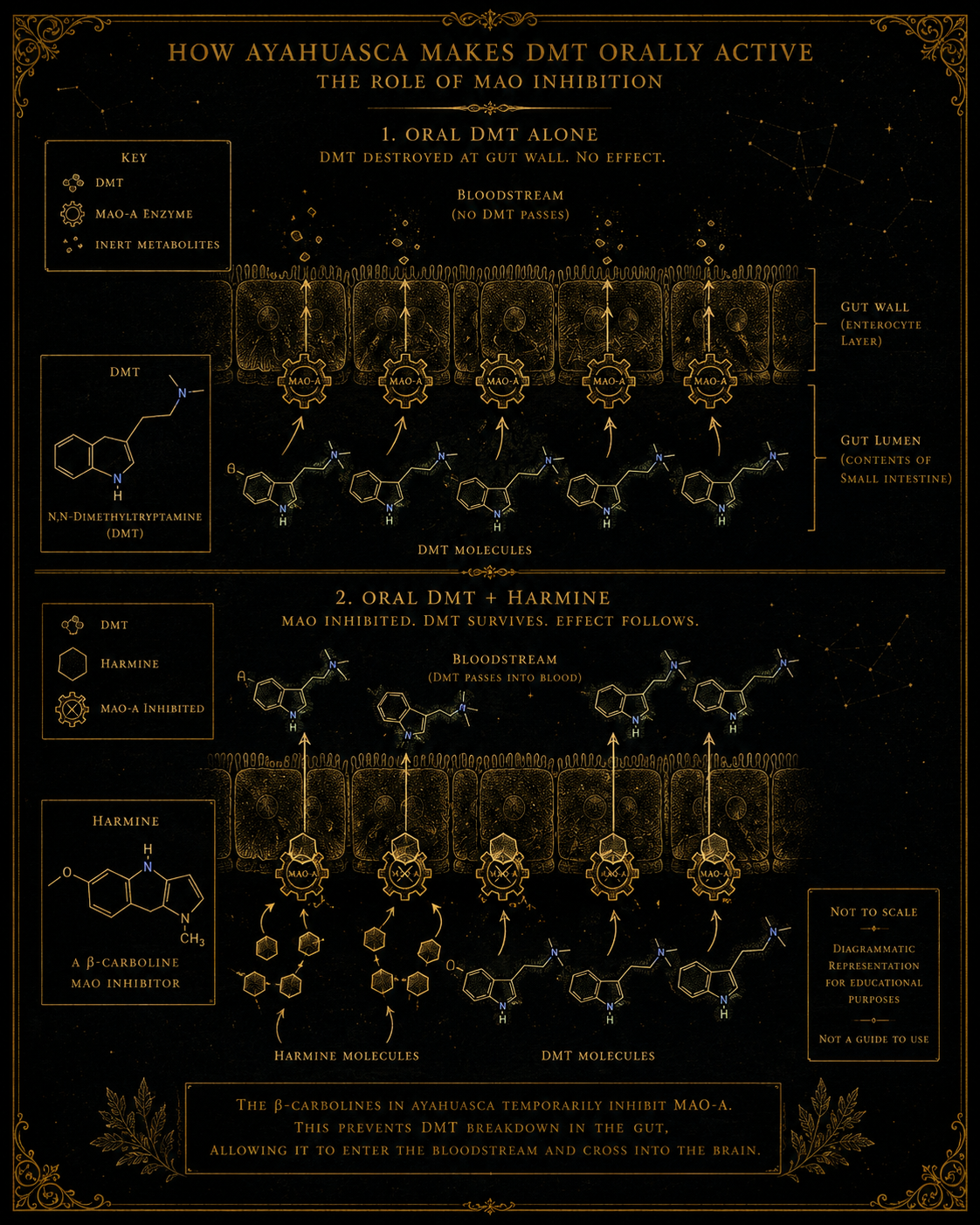
Oral N,N-DMT, taken on its own, reaches the gut wall, encounters intestinal MAO-A, and is broken down before it can be absorbed. Almost none reaches the bloodstream. The body's protection against dietary amines is, in this case, doing exactly its job. Oral DMT is pharmacologically inactive.
Combine the DMT with a sufficient quantity of harmine (and to a lesser extent harmaline and tetrahydroharmine), however, and the situation changes. The β-carbolines reach the gut wall first and inhibit the resident MAO-A. The DMT, taken alongside or shortly after, then survives intestinal transit. It is absorbed across the gut wall, enters the portal circulation, passes through the liver (where the same β-carbolines also inhibit MAO-A), reaches systemic circulation, crosses the blood-brain barrier, and reaches 5-HT2A receptors in the cortex. The active experience follows.
The duration is meaningfully extended by the same mechanism. Smoked DMT — which bypasses the gut entirely — reaches the brain in seconds and is cleared by the body's enzymes within minutes; the active experience lasts ten to twenty minutes. Oral DMT plus harmine takes thirty to sixty minutes to come on (because the DMT has to be absorbed first) and lasts four to six hours (because the MAO inhibition slows clearance throughout the experience). The pharmacology accounts cleanly for both differences.
There is a further subtlety worth registering. The β-carbolines are not pharmacologically inert beyond their MAO inhibition. They cross the blood-brain barrier themselves and have direct effects on serotonergic and other systems — effects that contribute, probably more than is sometimes acknowledged in popular discussion, to the overall ayahuasca experience. Experienced participants can sometimes distinguish vine-heavy brews from leaf-heavy ones by the quality of the experience alone. Whether this reflects different β-carboline:DMT ratios, the presence of admixture plants, or both is empirically debated.
6. The safety question
The safety profile of MAO inhibition is the most important practical material in this essay, and it deserves to be spelled out carefully rather than waved at.
The risk that does matter — and that has caused multiple documented deaths in connection with ayahuasca and other MAOI use — is the combination of MAO inhibition with other drugs that elevate serotonin. The class of concern includes:
- SSRIs (selective serotonin reuptake inhibitors) — fluoxetine, sertraline, citalopram, escitalopram, paroxetine, others
- SNRIs (serotonin-noradrenaline reuptake inhibitors) — venlafaxine, duloxetine, others
- Other MAOIs — including over-the-counter herbal products containing MAOI activity (St John's Wort is the most prominent example)
- Tramadol, pethidine, and several other opioids with serotonergic activity
- MDMA and related amphetamines
- 5-HT1A and 5-HT2A agonists more broadly — including, importantly, other psychedelics
Combination of MAOI with any of these can produce serotonin syndrome — a clinical emergency characterised by neuromuscular hyperactivity (tremor, hyperreflexia, clonus), autonomic instability (high temperature, blood pressure swings, sweating), and altered mental status. In severe cases it is fatal. Mild and moderate cases require prompt medical attention.
The risk is not merely theoretical. Case reports and safety reviews in the medical literature have identified serious adverse events in contexts where ayahuasca or MAOI-containing preparations were combined with serotonergic drugs. The precise causal role of any individual medication in adverse outcomes is often difficult to establish — ceremonies involve multiple variables — but the interaction risk is well enough characterised pharmacologically that reputable practitioners treat recent serotonergic medication use as a contraindication. Participants who do not disclose current medications, or who assume the combination is manageable, are taking a meaningful risk; this is not a theoretical pharmacology problem but a regularly recurring clinical concern.
Reputable practitioners require participants to discontinue serotonergic medications for an adequate washout period (typically four to six weeks for SSRIs, longer for some other classes) before a ceremony, and to remain off them for some days after. Commercial operators screen unevenly. Self-administered ayahuasca outside ceremonial settings is the highest-risk configuration, because the user is on their own to ensure that the medication-interaction problem has been adequately addressed.
The corollary worth stating clearly: anyone considering an encounter with ayahuasca (or with isolated harmine or any MAOI) who is currently taking, or who has recently taken, any of the medications above should regard this as a question that needs to be sorted out before — not during — any encounter. A primer is not the place to walk through specific medication-discontinuation protocols, which are individual to the person, the drug, the dose, and the indication.
A separate category of consideration: people with cardiovascular vulnerabilities. β-carbolines are mildly sympathomimetic — they can raise heart rate and blood pressure modestly — and the ayahuasca experience itself adds further cardiovascular load through the physical intensity of the vomiting, the sweating, and the prolonged altered state. Reputable retreat operators screen for cardiac risk factors; cardiac events at ceremonies, though rare, have occurred.
7. Harmine as an emerging research compound
This is the strand that has, in the last few years, become the most interesting development in the area — and the one that may eventually justify a separate Pillar essay rather than just a primer section.
Harmine, on its own, has properties that until recently received little attention beyond its role in ayahuasca. Several converging strands of preclinical research have changed that, and they share a common mechanistic thread worth introducing before walking through the specific applications.
DYRK1A: the target that made harmine interesting again
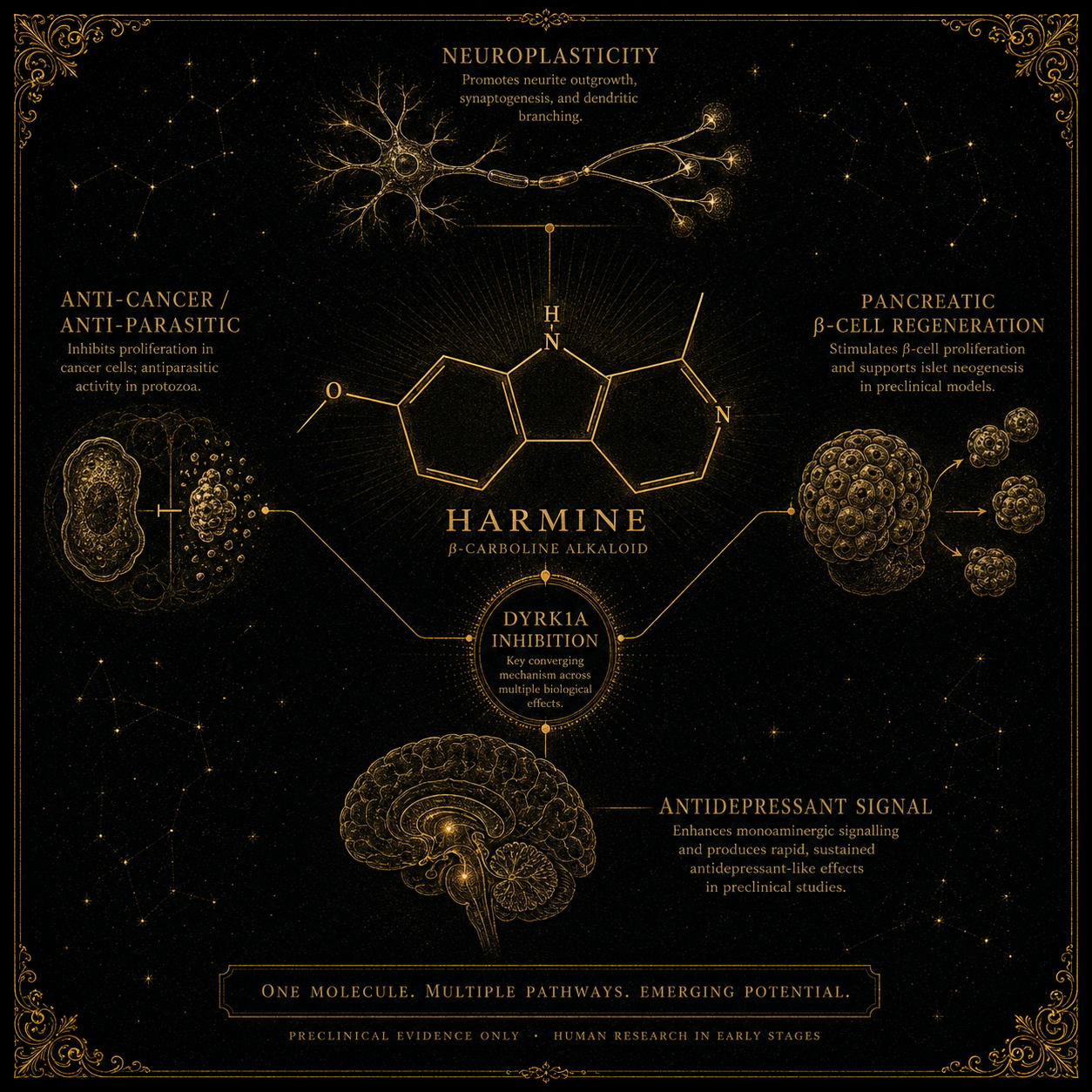
Much of harmine's emerging research profile traces back to one molecular target. DYRK1A is a kinase enzyme that, in its normal active state, holds various tissue types in their differentiated, non-proliferating condition. Inhibit DYRK1A and certain mature cell types regain a limited capacity to grow, divide, and form new connections — neurons can extend new synaptic branches, pancreatic β-cells can proliferate, and other regenerative effects become accessible. Harmine is among the best-known natural DYRK1A inhibitors, which is the unifying explanation behind several otherwise unrelated-looking research strands.
The converging clinical strands
A series of cell-culture and animal studies, beginning around 2019 and accelerating through the early 2020s, has demonstrated that harmine appears to promote the survival, growth, and development of human neurons. The findings have driven a steady increase in attention to harmine within the broader neuroplasticity research community. A separate strand of work, partly from the Mount Sinai laboratory of Andrew Stewart, has shown that harmine drives the proliferation of human pancreatic β-cells — the insulin-producing cells whose loss underlies type 1 diabetes and contributes to type 2. Harmine-based compounds for diabetes have entered early-stage human clinical investigation.
A third strand: multiple animal models, and a small number of early human pilot studies, suggest that harmine on its own may have antidepressant properties independent of any accompanying DMT. The mechanism is still being worked out — DYRK1A inhibition, MAO inhibition, neurogenesis-promoting effects, and direct serotonergic activity have all been proposed as contributors — but the convergent signal is genuine.
Beyond these three central strands, preclinical work has implicated harmine in possible therapeutic roles in Alzheimer's disease, certain cancers, parasitic infections, and several other contexts. Most of this remains at the bench rather than the bedside. None of it is established as clinical practice. But the aggregate picture is striking: a compound that has been known to humans for thousands of years as part of a ceremonial brew, dismissed pharmacologically for most of that time as "the MAOI in ayahuasca," is now being investigated as a potentially independent therapeutic agent in at least four distinct clinical contexts.
Why analogues may matter more than harmine itself
There is a subtlety here that often gets missed in the popular framing of "harmine the next antidepressant." The most likely future of this research strand is not harmine becoming a medicine — it is harmine teaching researchers how to design better molecules.
Harmine carries with it the MAO-inhibitor liability that makes it clinically awkward: the drug-interaction profile, the dietary considerations, the difficulty of combining it with most existing psychiatric medications. For a research compound, that liability is manageable. For a marketed pharmaceutical, it is a significant obstacle. Several pharmaceutical companies and research groups are therefore developing harmine analogues — modified versions of the molecule designed to retain the desirable properties (DYRK1A inhibition, neuroplasticity-promoting effects, β-cell proliferation) while reducing or eliminating the MAO activity.
If any of these analogues reaches medicine in the next decade, the contribution of harmine to that medicine will have been conceptual rather than literal: the natural compound will have served as a chemical template, identifying which receptor-and-enzyme interactions matter, and the molecule that actually reaches patients will be a synthetic refinement designed around those insights.
It is worth holding the irony lightly. The β-carbolines have been part of human pharmacology for at least 2,500 years through ayahuasca. Their independent therapeutic potential is being discovered now. The traditions that incorporated them into ceremonial practice did not need biochemistry to find out that they did something useful. The biochemistry is catching up.
8. Is it legal?
Harmine and the other β-carbolines occupy an unusual legal position compared with the substances covered in the previous primers.
United Kingdom. Harmine itself is not controlled under the Misuse of Drugs Act 1971 in the same way DMT is. Neither is Banisteriopsis caapi, nor Peganum harmala. What is controlled is ayahuasca as a preparation — the brew is treated as DMT for the purposes of the Act, regardless of the legality of its constituent plants individually, per the R v Aziz Court of Appeal decision. This does not, however, mean that harmine sits in a regulatory void: questions of supply, importation, intended use, product presentation, and the broader Psychoactive Substances Act 2016 may all matter in practice, and the absence of harmine from one schedule does not imply blanket permissiveness across the wider regulatory landscape.
United States. Federally, the same pattern: harmine is not on the Controlled Substances Act schedules. Neither is the vine or the seeds. Ayahuasca-as-brew falls under DMT scheduling.
Other jurisdictions. Most countries that prohibit ayahuasca do so on the DMT side rather than the β-carboline side. Some include harmine and harmaline on national lists; most do not.
The practical implication: the β-carbolines are widely accessible for research purposes, which is partly why the harmine-as-independent-therapeutic strand has been able to advance even in jurisdictions where ayahuasca remains controlled. The molecule that does the enzyme-inhibiting work in the brew can be studied in laboratories that could not legally hold the brew itself.
9. What people often get wrong
A handful of recurring confusions are worth addressing directly:
"The MAOI in ayahuasca just lets the DMT through. It does not do anything else." Partly true. The MAO inhibition is the necessary pharmacological enabling step; without it, the DMT is destroyed and the experience cannot happen. But the β-carbolines themselves cross the blood-brain barrier and have their own central effects — direct serotonergic action, mild cardiovascular effects, and probably contributions to the experiential quality of the brew that are not reducible to the DMT alone. Treating the vine as "just the carrier" understates what it does.
"Reversible MAOIs are safe with SSRIs because they are reversible." They are safer than irreversible MAOIs in some respects (dietary tyramine restrictions are looser; recovery is faster). They are not safe with SSRIs. The serotonin-syndrome risk from MAOI–SSRI combination is the issue, and it applies to reversible MAOIs as much as to irreversible ones, although the recovery window is shorter.
"Syrian rue and ayahuasca are pharmacologically equivalent." They share the β-carboline content, more or less, in different ratios. The DMT-containing plant they are combined with then determines the rest of the experience. Syrian rue plus a DMT-source plant produces a brew often called "anahuasca" or "pharmahuasca" — pharmacologically close to ayahuasca but lacking the cultural-ceremonial context. Whether the two are experientially equivalent depends entirely on what is being asked of the comparison.
"Harmine is a psychedelic." Not in the conventional sense. At doses present in ayahuasca, it is mildly psychoactive — some sedation, mild visual phenomena at the upper end — but it does not produce the classical psychedelic state. The classical psychedelic component of the ayahuasca experience is the DMT. The β-carbolines are doing other things.
"The traditional indigenous brewers were just lucky." Most ethnobotanists who have studied the question carefully reject this framing. The combination of MAO-inhibitor vine plus DMT-containing leaf, in the right ratios, brewed for the right duration, is a non-obvious pharmacological discovery. Whether it was reached through systematic trial and error, through plant-spirit communication (the traditional explanation), or through some combination of both, the result is more impressive than a lucky accident would account for. Treating the pharmacology as obvious or self-evident in retrospect overlooks how far ahead of contemporaneous Western pharmacology these traditions were operating.
10. What we still don't know
The unresolved questions in β-carboline research, briefly:
What the optimal harmine:DMT ratio is for producing the characteristic ayahuasca experience — and whether the traditional brews approximate that ratio by accident or by sophisticated empirical refinement.
How much of harmine's emerging therapeutic effects (in depression, in diabetes, in neuroplasticity) are mediated through DYRK1A inhibition versus its other activities, and whether selective DYRK1A inhibitors (without MAO activity) would retain the benefits.
Whether the cognitive and emotional sequelae often reported by ayahuasca participants in the weeks following a ceremony are attributable to the DMT, to the β-carbolines, to the ceremony itself, or to interactions between all three.
What role tetrahydroharmine (THH) plays in the experience — it is a serotonin-reuptake inhibitor as well as a weaker MAOI, and its contributions to the brew's effects are less well-characterised than harmine's.
Whether long-term repeated use of MAO-inhibitor-containing brews has any cumulative effects on neurotransmitter systems that have so far escaped clinical attention.
How the emerging clinical pipeline for harmine-based therapeutics will navigate the obvious tension between developing a compound's medical applications and the cultural framework that has held it for thousands of years as part of a sacred preparation.
These are the live questions. The answers to several of them are likely to land within the next decade.