ARDMT Field Notes
β-Carbolines and the MAO-A barrier: how ayahuasca makes oral DMT possible
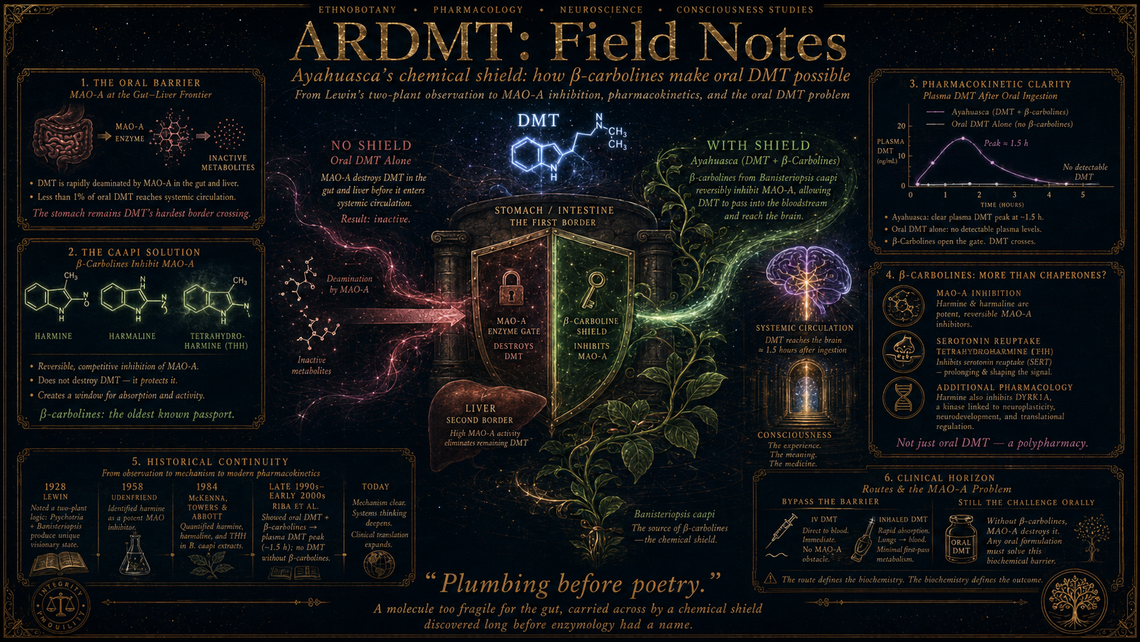
In 1928, when Lewin catalogued mescaline among his Phantastica, he noted something curious about ayahuasca: the brew required two plants, not one. A single plant supplied the visions, but without the other, swallowed on its own, the visionary substance did precisely nothing. The chemistry behind that observation would take another three decades to unravel, and when it did, the answer turned out to be less about the brain than about the gut.
DMT — N,N-dimethyltryptamine — is destroyed with ruthless efficiency by monoamine oxidase (MAO), particularly the MAO-A isoform lining the gastrointestinal tract and liver. Oral doses are deaminated before they ever reach systemic circulation. The indigenous preparation of ayahuasca solves this problem with Banisteriopsis caapi, a vine rich in β-carboline alkaloids — harmine, harmaline, and tetrahydroharmine — which are potent, reversible inhibitors of MAO-A. The combination is, in pharmacological terms, an oral delivery system of considerable elegance.
The work
The formal identification of harmine as a MAO inhibitor came relatively early. Udenfriend and colleagues at the National Institutes of Health demonstrated harmine's inhibition of MAO in vitro in 1958, working with rat liver homogenates and using serotonin as substrate. But the connection to ayahuasca's oral activity was not made explicit in Western pharmacology until the 1960s and 1970s, when ethnobotanists — most notably Richard Evans Schultes, and later Dennis McKenna — began articulating the two-component logic of the brew in biochemical terms.
The quantitative picture sharpened considerably with McKenna, Towers, and Abbott's 1984 paper in the Journal of Ethnopharmacology, which measured the β-carboline content of B. caapi and related species, reporting harmine concentrations of roughly 0.31–8.43 mg/mL in traditionally prepared decoctions. Harmaline typically appeared at lower concentrations, and tetrahydroharmine — a weaker MAO inhibitor but one present in substantial quantities — added a further pharmacological layer, as it also inhibits serotonin reuptake.
The critical human pharmacokinetic data arrived later still. Riba and colleagues in Barcelona, working through the late 1990s and early 2000s, administered freeze-dried ayahuasca capsules to volunteers at doses of 0.6 and 0.85 mg DMT/kg body weight. Plasma DMT levels peaked at approximately 1.5 hours, reaching roughly 12–17 ng/mL at the lower dose and proportionally higher concentrations at the upper dose. Without the β-carboline fraction, equivalent oral DMT doses produced no detectable plasma levels whatsoever. The monoamine oxidase barrier was, in effect, total.
What it changed
The β-carboline story did two things at once. First, it provided a pharmacological rationale for a centuries-old preparation — a rare instance in which indigenous technology preceded, and indeed predicted, the mechanistic explanation by several hundred years. Second, it opened a line of inquiry into whether the β-carbolines themselves contribute psychoactive or therapeutic effects beyond mere enzyme inhibition.
This second question remains genuinely unresolved. Harmine and harmaline have their own receptor pharmacology: affinity for imidazoline receptors, interactions at 5-HT₂A (though weak compared to DMT), and — in harmine's case — inhibition of dual-specificity tyrosine-phosphorylation-regulated kinase 1A (DYRK1A), a target of interest in neurogenesis and Down syndrome research. Tetrahydroharmine's serotonin reuptake inhibition raises the possibility that ayahuasca's subjective and neurobiological profile is not simply "oral DMT" but a polypharmacy whose components interact in ways that isolated DMT administration cannot replicate.
What remains
The current wave of clinical DMT research — intravenous infusions from programmes now under Cybin's umbrella, Algernon Pharmaceuticals' inhaled formulations, various extended-state IV protocols — deliberately bypasses the gut, rendering the β-carboline question moot for those programmes. Yet oral DMT formulations remain of interest, particularly for any future outpatient model in which intravenous access is impractical. The same MAO-A barrier that the caapi vine solved remains the central engineering problem.
Synthetic co-administration of harmine or pharmaceutical MAO inhibitors (iproniazid's descendants, as it were) is one approach; others have explored encapsulation technologies or prodrug strategies. Each carries its own safety calculus — reversible MAO-A inhibition with harmine is considerably more forgiving than irreversible inhibition, but tyramine interactions and serotonergic risks still demand careful dose-ranging.
The deeper pharmacological question — whether β-carbolines are mere chaperones or active participants — has implications for how faithfully any clinical DMT programme must reproduce the ayahuasca matrix to capture its reported antidepressant effects. One suspects the answer will prove to be: rather more faithfully than the current pipeline assumes.
Marginalia
It is a peculiar inversion: a molecule so fragile that the body destroys it on contact, wrapped in a chemical shield discovered empirically by cultures with no concept of enzymology. The stomach remains, for DMT, the hardest border crossing — and the β-carbolines, the oldest known passport.