ARDMT Field Notes
Why 0.4 mg/kg: Strassman's dose-finding logic and its thirty-year hold
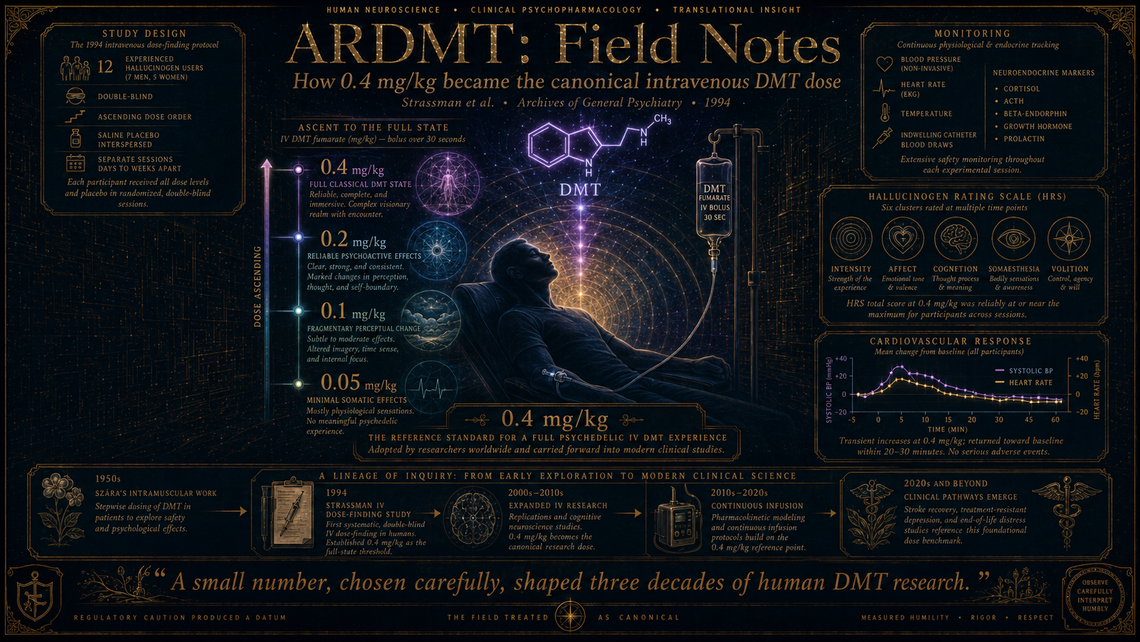
Rick Strassman's dose-finding logic in the 1994 intravenous DMT protocol is one of those stories best begun with a number: 0.4 mg/kg. It is a small figure, arrived at with considerable care, and it has quietly governed the design of human DMT studies for three decades. Nearly every modern intravenous DMT trial — from Imperial College's continuous-infusion work to the Algernon Pharmaceuticals stroke programme — calibrates itself, consciously or otherwise, against this value. How Strassman settled on it is a study in the practical ethics of psychedelic dose selection, conducted under constraints that would give most contemporary IRBs palpitations.
The story begins not in 1994 but in the late 1980s, when Strassman was assembling his Drug Enforcement Administration Schedule I licence and negotiating with the University of New Mexico's Human Research Review Committee. No one had administered DMT to a human volunteer under federal approval in the United States since the early 1970s. The regulatory ground was, to put it mildly, uncharted.
The work
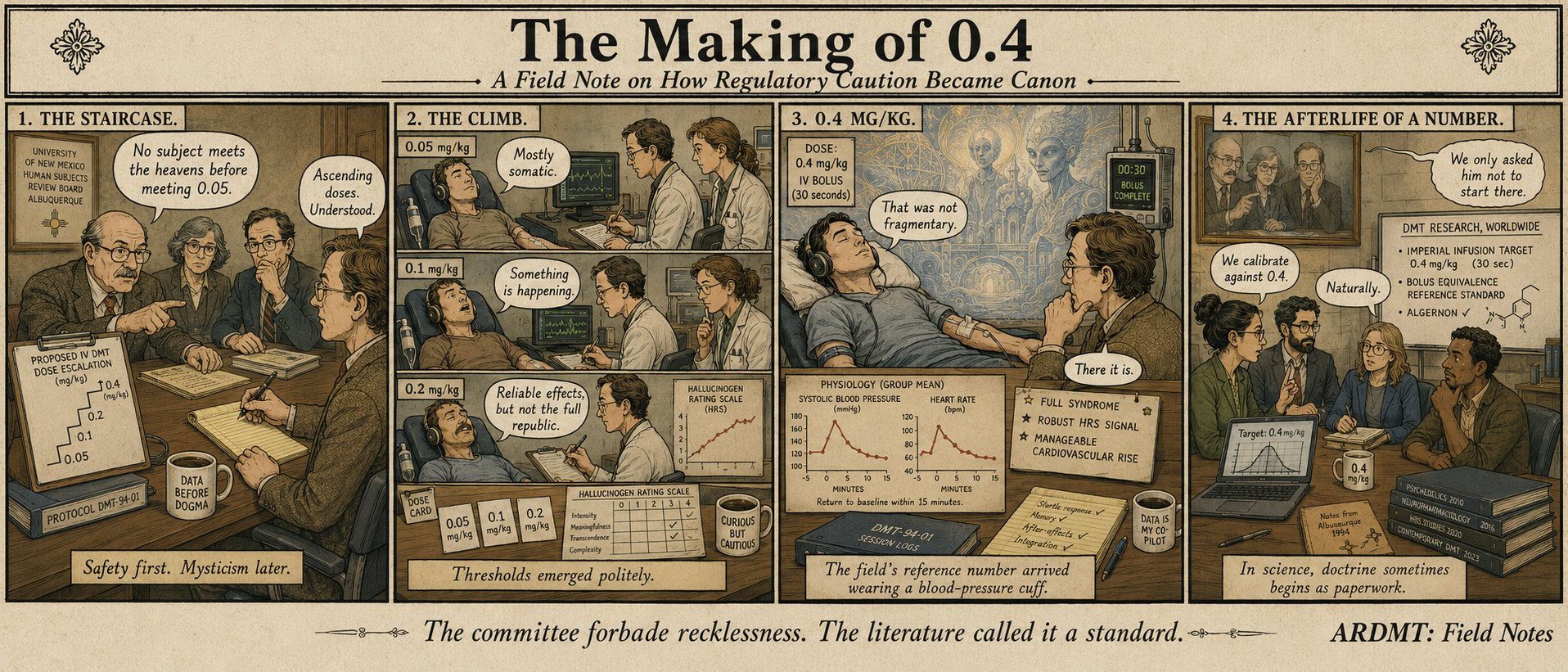
Strassman's dose-finding study, published in Archives of General Psychiatry in 1994, employed a double-blind design with four intravenous dose levels — 0.05, 0.1, 0.2, and 0.4 mg/kg of DMT fumarate — administered as bolus injections over 30 seconds. Twelve experienced hallucinogen users participated, each receiving all four doses in ascending order across separate sessions, with saline placebo interspersed. The ascending-dose structure was not arbitrary; it was a concession to safety. The committee required that no subject encounter a higher dose before tolerating a lower one without adverse event.
The pharmacological logic drew on two prior sources. The first was the Hungarian psychiatrist Stephen Szára's intramuscular work from the 1950s and 1960s, which had established a rough psychoactive threshold for DMT at approximately 0.7–1.0 mg/kg i.m. Strassman reasoned that intravenous delivery, bypassing the absorption lag of intramuscular injection, would require substantially less compound to achieve equivalent central effects. The second was the sparse animal literature on DMT's cardiovascular profile, which suggested a need for caution around blood pressure and heart rate at higher doses.
Cardiovascular monitoring was continuous: blood pressure, heart rate, and core temperature at fixed intervals. Neuroendocrine measures — β-endorphin, cortisol, prolactin, growth hormone, ACTH — were drawn via indwelling catheter. Subjective effects were captured by the Hallucinogen Rating Scale (HRS), an instrument Strassman himself developed for the study, having found existing psychometric tools inadequate to the phenomenology.
At 0.05 mg/kg, subjects reported little beyond mild somatic sensation. At 0.1 mg/kg, perceptual changes emerged but remained fragmentary. The 0.2 mg/kg dose produced reliable psychoactive effects in most subjects — visual imagery, altered time perception, affective shifts — but the full classical DMT state, with its characteristic immersive visions and sense of entering an autonomous space, emerged consistently only at 0.4 mg/kg. This dose also produced the most robust neuroendocrine signal: significant elevations in β-endorphin, corticotropin, cortisol, and growth hormone, with prolactin notably unaffected — a finding Strassman interpreted as evidence against primary dopaminergic mediation of the acute response.
Blood pressure rose at 0.4 mg/kg — mean arterial pressure increased meaningfully within two minutes of injection — but returned to baseline within fifteen minutes. No subject required intervention.
What it changed
The 0.4 mg/kg dose became, in effect, the field's reference standard for a "fully psychedelic" intravenous DMT experience. Strassman used it as the anchor dose in his subsequent extended study of sixty volunteers, and when other groups began working with intravenous DMT years later, they inherited the figure. Christopher Timmermann's continuous-infusion work at Imperial, for instance, uses a bolus-plus-infusion protocol designed to sustain plasma levels equivalent to the peak achieved by Strassman's bolus. The number 0.4 is the gravitational centre.
Equally influential was the HRS, which provided the first standardised vocabulary for quantifying the DMT state. Its six clusters — Intensity, Affect, Cognition, Perception, Somaesthesia, Volition — remain in wide use, though subsequent instruments have supplemented them.
What remains
The ascending-dose, within-subjects design made practical sense in 1994, but it confounded dose with expectation and order effects — a point Strassman acknowledged. Modern dose-finding studies, such as those in the psilocybin literature, more commonly use randomised dose-order designs with washout periods, though DMT's short duration makes the comparison imperfect. The question of whether 0.4 mg/kg is optimal or merely sufficient has never been formally re-examined; it has been accepted largely on the strength of Strassman's clinical observation that it reliably produced the full syndrome without unmanageable cardiovascular risk. Whether lower doses might serve therapeutic purposes — a question now live in the context of Algernon's stroke work and Cybin's depression programme — requires a different kind of dose-response analysis than Strassman's study was designed to provide.
Marginalia
There is something faintly comic about the fact that the most consequential number in human DMT research was chosen, in part, because a committee in Albuquerque would not permit Strassman to start at a higher dose and work down. Regulatory caution produced a datum the field has treated as canonical ever since. One suspects the committee would be surprised.