ARDMT Field Notes
Deuterating DMT: how two neutrons reshape a pharmacokinetic profile
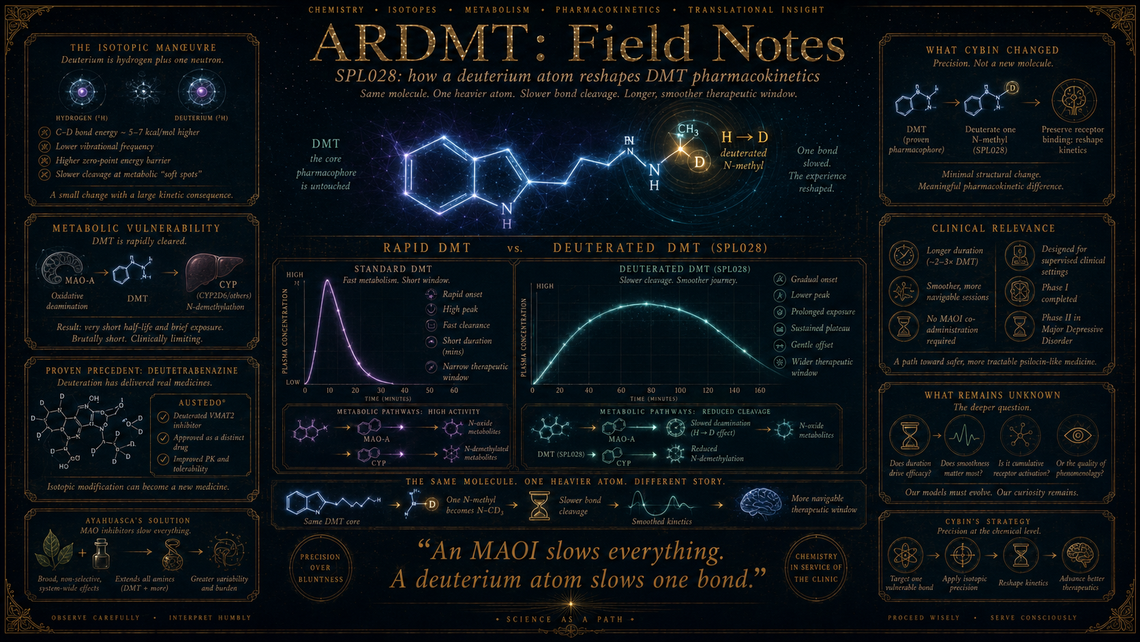
When Cybin Inc. filed its patent family around CYB003 — later redesignated SPL028 — the core chemical manoeuvre was, on its face, almost comically modest. The company had taken N,N-dimethyltryptamine, a molecule whose basic structure had been known since Manske synthesised it in 1931, and replaced two hydrogen atoms on one of its methyl groups with deuterium. That is all. The carbon skeleton remained untouched. The pharmacophore was unchanged. The indole ring, the ethylamine chain, the two N-methyl groups: all present and correct. The alteration was isotopic, not structural — a substitution visible only to a mass spectrometer. Yet this small swap, amounting to roughly two atomic mass units on a molecule weighing 188 daltons, was expected to meaningfully alter the drug's behaviour in a living body. Understanding why requires a short detour into bond physics, and from there into the particular metabolic vulnerabilities of tryptamines.
The work
Deuterium is hydrogen with an extra neutron: same electron count, same chemistry at equilibrium, but a carbon–deuterium bond vibrates at a lower frequency than a carbon–hydrogen bond and, critically, presents a higher zero-point energy barrier to cleavage. The practical consequence is that enzymes which break C–H bonds — notably the monoamine oxidases and cytochrome P450 isoforms responsible for tryptamine metabolism — find C–D bonds somewhat harder to sever. The rate reduction is not dramatic in most contexts; the primary kinetic isotope effect for C–H versus C–D cleavage is typically a factor of two to seven, depending on whether the bond-breaking step is fully rate-limiting. But for a molecule like DMT, whose clinical pharmacology is almost entirely governed by how fast it is destroyed, even a two-fold change in metabolic rate can reshape the entire pharmacokinetic profile.
DMT's central pharmacokinetic problem has been well documented since Szára's early self-experiments in the 1950s: the molecule is an excellent substrate for monoamine oxidase A (MAO-A), which oxidatively deaminates the ethylamine side-chain, and for various cytochrome P450 enzymes that perform N-demethylation. Intravenous DMT is cleared from plasma in minutes; the subjective experience, while intense, is brutally short. Oral DMT is destroyed almost entirely on first pass through the gut wall and liver, which is why ayahuasca traditions co-administer β-carboline MAO inhibitors. The molecule's therapeutic window — the range of plasma concentrations at which effects are sustained long enough to be clinically useful without provoking overwhelming perceptual disruption — is, accordingly, narrow and fleeting.
Cybin's strategy with SPL028 was to deuterate one of the N-methyl groups, specifically targeting the site most susceptible to CYP-mediated N-demethylation. By slowing this particular metabolic step, the aim was not to create a different drug in the pharmacodynamic sense — SPL028 should, in principle, bind 5-HT₂A receptors with essentially the same affinity as DMT, since the receptor-binding interaction involves the indole ring and the protonated amine, neither of which is altered — but to produce a molecule with a gentler pharmacokinetic curve: slower onset, longer plateau, smoother offset. The clinical hypothesis is that this profile would prove more tractable in a supervised therapeutic setting than the vertiginous bolus kinetics of intravenous DMT.
What it changed
Deuteration as a pharmaceutical strategy was not new to Cybin. Concert Pharmaceuticals (now part of Sun Pharma) had applied the approach with deutetrabenazine (Austedo), approved by the FDA in 2017 for Huntington's chorea and tardive dyskinesia — a deuterated version of tetrabenazine with improved half-life and reduced dosing frequency. That approval validated the regulatory principle that an isotopic modification could constitute a distinct drug with a distinct clinical profile, even when the pharmacophore was unchanged. Cybin's application of the same logic to a tryptamine psychedelic was, in that sense, a straightforward extension of an established platform.
What made it rather more interesting — and rather more uncertain — was the question of whether psychedelic pharmacology would respond to kinetic smoothing in the same way that a VMAT2 inhibitor did. DMT's subjective effects are notoriously non-linear with respect to plasma concentration; there is some evidence, from Strassman's dose-ranging work in the 1990s and from more recent continuous-infusion studies such as those by Timmermann and colleagues, that the quality and not merely the intensity of the experience shifts as the rate of onset changes. A slower rise might not simply produce a gentler version of the same experience; it might produce a qualitatively different one. One suspects the phenomenology will prove at least as important as the kinetics, though disentangling the two will be decidedly non-trivial.
What remains
SPL028 has moved through Phase I and into Phase II clinical trials for major depressive disorder, with Cybin reporting tolerability data that appear consistent with the intended pharmacokinetic reshaping — a longer duration of acute effect relative to intravenous DMT, without the need for MAO inhibitor co-administration. The deeper question, however, is whether kinetic profile per se is a therapeutically meaningful variable, or whether the critical mediator of antidepressant effect is cumulative 5-HT₂A receptor activation (an area-under-the-curve argument), peak receptor occupancy (a Cmax argument), or something else entirely — perhaps the subjective phenomenology itself acting as an active psychological ingredient. The deuteration strategy makes an implicit pharmacological bet: that duration and smoothness matter. Whether that bet is correct will require controlled comparisons not merely against placebo but against DMT itself — a head-to-head design that, to date, no trial appears to have attempted.
The broader implication is methodological. If deuteration can selectively tune tryptamine kinetics without altering receptor binding, the approach opens a combinatorial space: different sites of deuteration, different degrees of metabolic retardation, potentially a menu of DMT-derived molecules each with a distinct temporal signature. The molecule becomes, in a sense, a platform rather than a drug. Whether that space is genuinely worth exploring, or whether the differences between variants prove clinically negligible, remains an open question — but it is a genuinely interesting one.
Marginalia
There is something faintly paradoxical about spending millions of dollars and several years of regulatory effort to make a molecule do what Amazonian ayahuasqueros accomplished centuries ago with a second plant — namely, slow down DMT's metabolism long enough for it to be useful. The difference, of course, is specificity: an MAO inhibitor slows everything; a deuterium atom slows one bond. Whether that precision justifies the enterprise is a question the clinic, not the chemistry, will eventually have to answer.