ARDMT Field Notes
Szára's 1956 self-experiment: the Budapest dose that launched DMT research
It is a quiet day on the wires, which suits us well enough, because it gives occasion to return to Budapest in 1956 and to a young psychiatrist doing something that, by any modern reckoning, was either admirably rigorous or mildly insane — and quite possibly both at once.
Szára's Self-Experiments: The Dose That Opened a Field
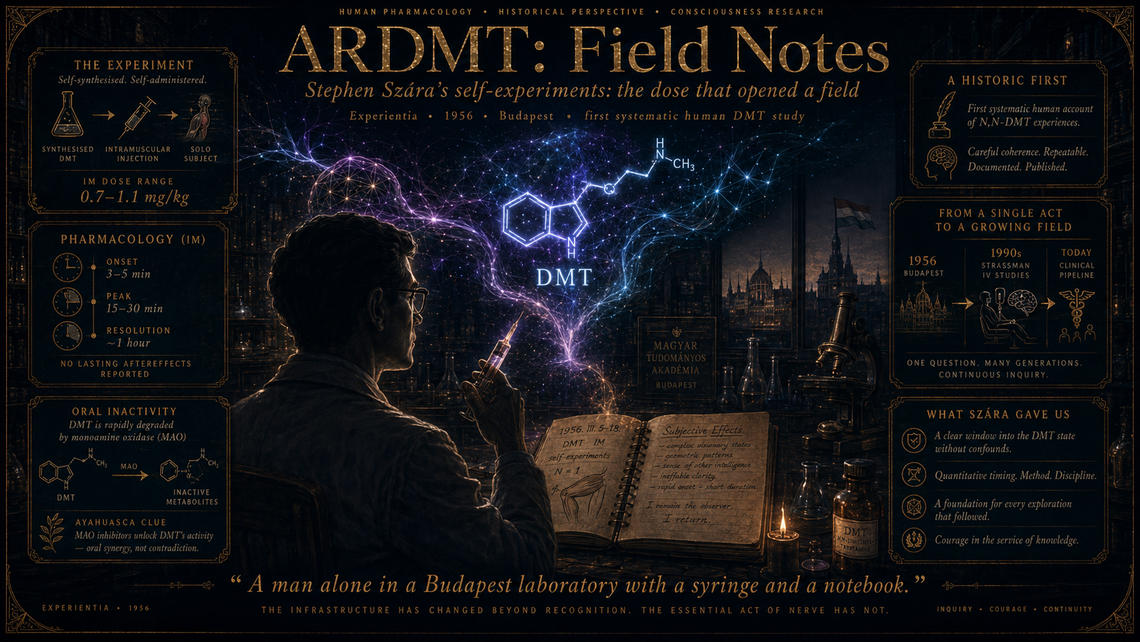
Stephen Szára had read the literature on mescaline and LSD with the keen attention of a researcher who sensed that something important was afoot in the indolealkylamines, and who also happened to be working behind the Iron Curtain, where Sandoz was disinclined to post free samples of lysergic acid diethylamide. Unable to procure LSD, he did what a certain kind of mid-century pharmacologist considered the obvious next step: he synthesised N,N-dimethyltryptamine himself, and then — finding no volunteers whose informed consent would have satisfied even the relaxed ethical norms of the era — injected it intramuscularly into his own deltoid.
The results, published in Experientia in 1956 and expanded upon in subsequent papers, constitute the first systematic account of DMT's psychoactive effects in humans. Szára administered doses ranging from roughly 0.7 to 1.1 mg/kg intramuscularly to himself and, eventually, to a small group of physician-volunteers. He documented onset within three to five minutes, a peak at around fifteen to thirty minutes, and near-complete resolution within an hour — a pharmacokinetic profile that remains, nearly seventy years on, essentially undisputed. He described vivid visual hallucinations, alterations in spatial perception, euphoria, and what he termed "a feeling of extraordinary significance," a phrase that anyone who has since read a trip report will recognise as a masterpiece of understatement.
What makes Szára's work more than a charming historical curiosity is the precision of his observations and the questions they implicitly raised. He noted the compound's failure to produce effects when taken orally — a finding that would later be explained by monoamine oxidase degradation in the gut and liver, and that simultaneously accounted for why ayahuasca traditions had long combined DMT-containing plants with MAO-inhibiting admixtures. He recorded dose-response relationships, onset and offset times, and qualitative phenomenological descriptions that, while necessarily subjective, were structured with clinical discipline. He was, in short, doing Phase I human pharmacology in a political context where institutional oversight was minimal and personal risk was the entry fee.
The significance of the 1956 work ripples forward in several directions. First, it established DMT as a compound of legitimate psychiatric interest rather than a mere chemical curiosity, setting the stage for the "endogenous psychotogen" hypothesis that would preoccupy researchers through the 1960s and 1970s — the notion, still not entirely settled, that DMT produced naturally in the human body might play some role in psychosis, dreaming, or near-death states. Second, Szára's intramuscular route of administration remained the standard for human DMT research until Rick Strassman's intravenous work at the University of New Mexico in the 1990s, which was explicitly modelled on, and indebted to, Szára's protocols. Third, the sheer brevity of the DMT experience that Szára documented — an intense psychedelic episode lasting less than an hour — is precisely the property that has made the molecule attractive to contemporary clinical programmes exploring DMT for treatment-resistant depression, where a short-acting compound offers practical advantages over the sprawling eight-hour commitment of a psilocybin session.
There is also something instructive, perhaps cautionary, in the fact that Szára's self-experimentation was born of geopolitical constraint. He could not get LSD, so he made DMT. Science, as ever, follows the path that circumstance permits, and the molecules we study are shaped as much by supply chains and customs regulations as by rational pharmacological priority-setting. One wonders what alternative history would have unfolded had Sandoz been rather more generous with its Eastern Bloc mailing list.
Szára went on to a long and distinguished career at the National Institute on Drug Abuse in the United States, eventually becoming chief of its biomedical research branch. He remained interested in tryptamines throughout his life and lived long enough to see the renaissance of psychedelic research that his early work had helped, in its modest way, to seed. He died in 2014, aged ninety, having outlived the Cold War, the War on Drugs, and the long prohibition-era silence that separated his experiments from their intellectual descendants.
Marginalia. The modern DMT clinical pipeline — extended-state infusions, EEG-monitored dosing, carefully titrated protocols — traces its genealogy to a man alone in a Budapest laboratory with a syringe and a notebook. The infrastructure has changed beyond recognition. The essential act of nerve has not.