Research
SPL028 Cybin 2024
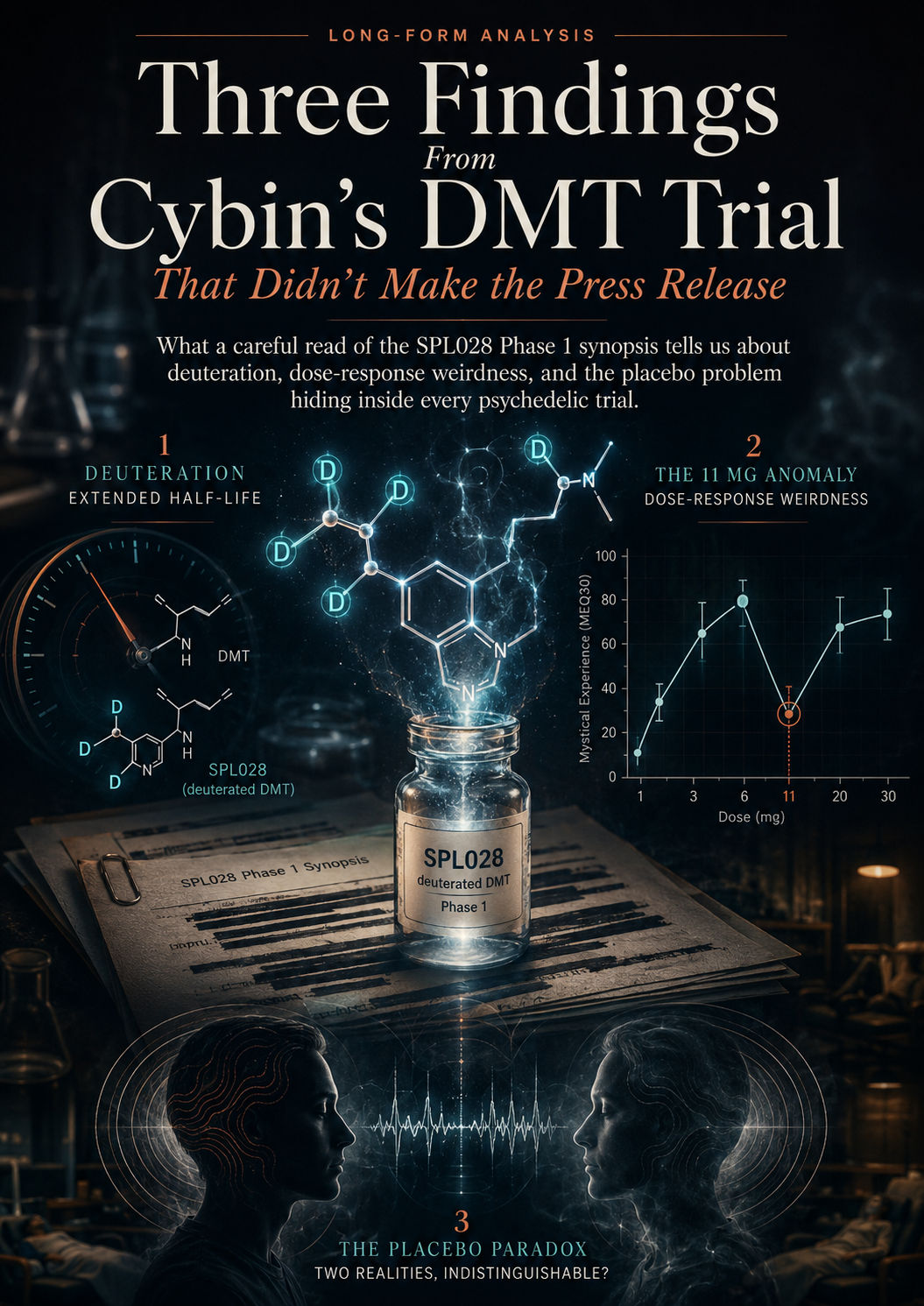
Three Findings From Cybin's DMT Trial That Didn't Make the Press Release
What a careful read of the SPL028 Phase 1 synopsis tells us about deuteration, dose-response weirdness, and the placebo problem hiding inside every psychedelic trial.
In December 2024, a Phase 1 trial synopsis was quietly filed to the ISRCTN registry. It described twelve months of healthy-volunteer dosing in Manchester of a molecule called SPL028 — a chemically engineered version of DMT that the sponsor, Small Pharma (now Cybin), believes could become the first commercially viable short-acting psychedelic medicine.
The press-release version of this story is short and clean. SPL028 was well tolerated. The pharmacokinetics worked. Higher doses produced complete mystical experiences. Onward to Phase 2.
The synopsis tells a more interesting story. Three of them, actually.
In the short-form pieces I've been making about this trial, I've pulled each thread separately. This is where they come together — with the context, the caveats, and the bits that don't fit into a 60-second reel.
What SPL028 actually is, and why this trial matters
DMT — N,N-dimethyltryptamine — is the most pharmacologically intense psychedelic ever studied in humans. Administered intravenously, it produces a complete, immersive psychedelic state within about two minutes and resolves within fifteen to thirty. That short duration is part of what makes it scientifically interesting: a clinician can observe the entire pharmacological window in a single afternoon.
It's also what makes it commercially difficult. Most psychedelic therapy models, from psilocybin onward, rely on a long enough drug experience to build a structured therapy session around. A fifteen-minute experience doesn't fit that model.
Small Pharma's bet was to fix this with chemistry rather than dose. They modified the DMT molecule by replacing two hydrogen atoms at the alpha-carbon with deuterium — a stable, heavier isotope of hydrogen. Deuterium forms slightly stronger bonds with carbon than ordinary hydrogen does, and those bonds are harder for liver enzymes to break. The drug is functionally the same; it just survives metabolism for longer.

This is not a new pharmaceutical strategy. Deutetrabenazine, sold as Austedo, is a deuterated version of tetrabenazine used to treat the chorea of Huntington's disease. The deuteration roughly doubled the half-life and allowed the drug to be dosed less frequently, which earned it a fresh patent and FDA approval in 2017. The technique is well-established. What SPL028 does is apply it to a psychedelic.
If it works, you don't get a different drug. You get DMT that lasts long enough to do therapy with.
The Phase 1 trial reported in this synopsis is the first human safety data on whether the technique held up.
Finding one: the deuteration story actually worked
Buried in the conclusions section of the synopsis is this sentence: “SPL028 IV half-life was approximately 3-times longer than IV DMT, demonstrating a robust kinetic isotope effect via deuteration of the DMT α-carbon.”
This is the technical confirmation that the chemistry achieved its goal. SPL028, given intravenously, persists in plasma roughly three times as long as ordinary IV DMT. The deuterium did its job.
Two practical consequences follow.
The first is that the dosing window changes. The synopsis describes participants spending the duration of the experience in a calm, prepared room, with eye shades and headphones, encouraged to focus inward. That's a setting designed for a therapeutic experience, not a brief pharmacological flash. A fifteen-minute drug doesn't really need this kind of preparation infrastructure. A forty-five minute one does, and crucially, can be built around it.
The second is that the intramuscular route becomes meaningful. This trial tested both IV infusion and IM injection — and the IM injection produced a delayed Tmax of ten to twenty minutes compared to the IV route, with a mean residence time approximately 1.5 times longer than the IV infusion. That difference matters commercially. IV dosing requires cannulation, infusion pumps, and trained staff. IM injection is something that can be done in a treatment chair with no special equipment. If SPL028 IM proves out in Phase 2, the deployment model is much more like a primary-care injection than a hospital infusion. This is the most commercially significant finding in the trial that isn't being talked about anywhere I've seen.
The MEQ data supports the broader case. The Mystical Experience Questionnaire is a thirty-item instrument scored on a percentage scale, and a score of sixty percent or above is treated in the literature as a "complete mystical experience" — a threshold that correlates, in psilocybin research, with later antidepressant response. In this trial, the 17 mg IV, 20 mg IM, and 30 mg IM cohorts all crossed that threshold. So did the 9 mg IV cohort, which is interesting for reasons we're about to come to.
If you're willing to take the MEQ as a meaningful surrogate endpoint — and that's a real if, which I'll come back to — then SPL028 produces, in healthy volunteers, the kind of subjective experience that has been associated with therapeutic benefit elsewhere. The pharmacology works. The chemistry works. The clinical setup works.
That's the easy story.
Finding two: the 11 mg dose anomaly
Now it gets weirder.
The trial dosed five active groups across the IV and IM routes: 9 mg IV, 11 mg IV, 17 mg IV, 7.5 mg IM, 15 mg IM, 20 mg IM, and 30 mg IM. Cohorts 1 and 2 received both an IV dose and an IM dose across two treatment periods. Cohorts 3, 4, and 5 received only one route.
A normal dose-response curve for a psychedelic looks like: more drug, higher peak plasma concentration, stronger subjective effects, more participants crossing the mystical experience threshold. Within reason and within the safety window, this is what you expect.
The 11 mg IV dose did not behave that way.
According to the synopsis, the 11 mg IV dose produced a lower mean Cmax, AUC-last, and AUC-inf than the 9 mg dose. On the subjective measures, Cohort 2 (11 mg IV) scored below Cohort 1 (9 mg IV) on the MEQ, the EDI (ego dissolution), the EBI (emotional breakthrough), the CEQ (challenging experiences), the IRVAS (intensity rating), and the VAS items. On essentially every measure that mattered, a higher dose produced a weaker effect.
The synopsis itself flags this as "surprising" and offers three candidate explanations: small sample sizes, individual variability in physiology and blood flow, and timing differences in PK sampling. None of these are conclusive. The honest reading is that the trial doesn't know why this happened.
It's worth dwelling on what a Phase 1 cohort actually is, because this is where the limitations of the data become important. Each cohort in this trial was six participants. A finding based on six people, even with careful sampling, is fragile. The 11 mg vs 9 mg comparison may be a real signal — perhaps a metabolic quirk specific to that batch of participants, perhaps a sampling artefact, perhaps something about the formulation or the infusion. Or it may be statistical noise that disappears with larger numbers.
What it is not is an indictment of the drug. The 17 mg IV dose performed as expected, with the highest dose-normalised Cmax and the highest MEQ scores. The dose-response works at the higher end. The 11 mg point is an anomaly in the curve, not evidence the curve doesn't exist.
But it does illustrate something important about how Phase 1 trials work, and how their results get reported. The press-release version of this trial will describe a clean dose-response relationship. The synopsis describes a messy one with a question mark in the middle of the IV range. Both are technically true depending on what you choose to mention.
This is the kind of detail that matters for understanding where the field actually is. Psychedelic trials are still small, still early, still producing the kind of data where individual outliers can swing a cohort mean. Anyone treating Phase 1 mystical experience scores as established efficacy is reading more confidence into the numbers than the numbers can carry.
Finding three: the placebo paradox
This is the one I want to spend the most time on, because it's the most interesting finding in the synopsis and it's the one almost no coverage will pick up.
The trial design for Cohorts 1 and 2 had two treatment periods separated by a washout of three to six weeks. Some participants in each cohort received SPL028 in TP1 and placebo in TP2, or vice versa, in a double-blind crossover. Cohorts 3, 4, and 5 each had only one treatment period.
This created two different placebo populations whose responses can be compared.

Group A — participants in Cohorts 1 and 2 who received placebo. By the time they got that placebo dose, they had already received an active dose of SPL028 a few weeks earlier in TP1. They had felt the drug.
Group B — participants in Cohort 4 who received placebo. They had never received SPL028. The placebo was their only dose.
The comparison the synopsis makes between these two groups is buried in the PD Results section, but it's striking.
On the Emotional Breakthrough Inventory, Group A scored higher than Group B. The synopsis explicitly notes this: the previously-dosed placebo group experienced a stronger placebo effect than the never-dosed placebo group.
On the IRVAS — the Intensity Rating Visual Analogue Scale — Group A again scored higher than Group B.
On the VAS items, Group A's scores tended to be higher than Group B's.
And on some of these subjective measures, Group A — placebo, but with prior active drug exposure — scored higher than Cohort 4 receiving the active 17 mg IV dose.
Read that again. People who received saline, but who had previously received the actual drug a few weeks earlier, reported subjective experiences in some respects more intense than people receiving the highest IV dose for the first time.
The synopsis's framing is cautious — “suggesting that the psychedelic-experienced cohort experienced a stronger placebo effect” — but the implication is significant. Prior exposure to a psychedelic state appears to amplify the response to a subsequent placebo. The brain, having once gone there, can be more easily induced to revisit something resembling the territory.
This is not a new idea in the literature. Expectancy effects in psychedelic trials are a known and growing concern. Researchers including Balázs Szigeti and Boris Heifets have argued that the placebo response in psychedelic studies is large, modifiable, and partly a function of participants' prior exposure and beliefs. What this synopsis does is provide one more data point in that argument — and a particularly clean one, because the comparison is within a single trial, with the same drug, the same protocol, and the same setting.
Two implications follow.
The first is methodological. Crossover designs in psychedelic trials, where the same participant receives both active drug and placebo, may systematically inflate placebo responses in the second period. If you're trying to measure drug-versus-placebo difference, a participant who has already had the drug isn't a clean placebo control. The field has known this in principle. This data shows it in practice.
The second is more philosophical. If a substantial portion of the subjective psychedelic experience can be reproduced — at least in some participants, on some measures — by an inert injection in a prepared setting after prior exposure, then the question of what is actually doing the therapeutic work becomes harder to answer. Is it the drug? Is it the state the drug induces? Is it the conditioning of having entered that state once? Is it the setting, the preparation, the integration session?
These are not new questions, but the SPL028 data sharpens them.
I want to be careful not to overclaim here. Six participants in each cohort. One trial. Healthy volunteers, not patients. The finding is signal, not proof. But it's signal that aligns with a growing body of methodological concern in the field, and it deserves more attention than the press cycle is going to give it.
What the redactions tell us
The version of this synopsis that's publicly available has several passages blacked out. The redactions appear to cluster around specific PK parameters — half-life values, plasma concentration ranges, and details about the volume of distribution. There's also redaction in the safety narrative around Cohort 4, the 17 mg IV group.
There are a few likely reasons for redactions of this kind. The most common is commercial sensitivity: PK parameters are competitively useful information for other companies developing similar drugs, and sponsors will often redact them in pre-publication releases. Some redactions may relate to ongoing patent or intellectual property considerations. Some may be safety-related, in the sense that specific values are still under regulatory review.
What you can read from the pattern is that Cybin has chosen to release the structure of the trial and the directional findings — half-life roughly tripled, doses tested, mystical experience thresholds crossed — while withholding the specific numerical values that a competitor would need to replicate the work. That's a normal commercial choice. It's worth knowing it's happening, because it means the public version of the trial is, by design, less informative than the version regulators see.
What this trial actually tells us
To pull the threads together.
SPL028's deuteration strategy works. The half-life is meaningfully extended. The drug is well tolerated within the dose range tested, with the caveats that the 17 mg IV cohort had two participants whose infusions were stopped early due to side effects, and that one participant had a severe psychomotor hyperactivity event. The dose ceiling is being probed and is real.
The dose-response curve is roughly as expected at the top end but has an unexplained dip at 11 mg IV that the trial itself can't account for. This is a Phase 1 reality, not a deal-breaker, but it's a flag.
Higher doses across both routes produced complete mystical experiences as measured by the MEQ — but the placebo data should make us cautious about how much of that response is being driven by the drug versus by expectation, conditioning, and setting.
The IM route works. Onset is delayed by ten to twenty minutes versus IV but the experience occurs and the safety profile is comparable. The path to a real-world clinic deployment, if SPL028 IM proves out in Phase 2, looks dramatically more practical than for IV-only protocols.
What this trial does not tell us is whether SPL028 treats depression, or any other psychiatric condition. This was a Phase 1 healthy-volunteer trial. The MEQ scores are a predictor researchers associate with antidepressant response in other compounds. They are not, in themselves, a measure of efficacy. Phase 2 trials in patient populations will start to answer that question. Part B of this same protocol — the open-label patient cohort — is where that data will come from.
What to watch next
For DMT and DMT-adjacent compounds specifically, the next twelve to eighteen months are going to be busy.
Cybin is expected to move SPL028 into Phase 2 work in major depressive disorder. The Part B data, when it appears, will be the first real efficacy signal from this molecule.
Beckley Psytech's BPL-003 — an intranasal formulation of 5-MeO-DMT, a related but pharmacologically distinct molecule — has Phase 2b data emerging in treatment-resistant depression. This is currently the most advanced near-term DMT-family compound and the readout is one to watch closely.
GH Research's GH001, an inhaled 5-MeO-DMT, is also in Phase 2 work in treatment-resistant depression with results expected over the next year.
For ibogaine, the ongoing observational work at Ambio Life Sciences and the Stanford ibogaine for traumatic brain injury research are the two most credible threads. Ibogaine is a different beast pharmacologically — a long-duration, cardiotoxic experience with very different scheduling and regulatory considerations — and worth tracking on its own track.
I'll be covering each of these as they develop. The short-form versions appear on the social channels. The long-form analysis — the version where I can actually pull the threads together — lives here.
A note on how I read these documents
One thing worth flagging, partly as transparency and partly because it's useful for anyone who wants to read trial documents themselves.
Phase 1 synopses use a specific vocabulary that signals where the interesting parts are. Words like surprising, unexpected, in contrast, however, and despite almost always mark a finding that the authors themselves consider anomalous. A keyword search for those terms across any synopsis is one of the fastest ways to surface the buried findings. The 11 mg anomaly and the placebo finding both came from sentences containing those flag words.
Equally, the structure of these documents matters. The conclusions section is usually a sanitised summary. The PK Results and PD Results sections are where the actual findings live, often in dry language that doesn't flag itself as important. The interesting bits sit several pages into the document, written in the same neutral tone as everything around them, easy to skim past.
Reading carefully takes longer than reading the press release. It's also where everything actually is.
Source: Clinical Study Report CT028_001, MAC Number: MAC 150, Final Version 1.0, 02 December 2024. ISRCTN registry: ISRCTN42293056. Sponsor: Small Pharma Ltd (now Cybin Inc.).
Next breakdown: [name the next compound or trial here]. Subscribe to get it in your inbox.