Foundations
Holding the Door Open

Extended-state DMT (DMTx): how scientists learned to hold a five-minute breakthrough open — what it is, what it has actually shown, and what is being sold on top of it
Start here: the whole thing in a paragraph
For seventy years, the strangest reliable experience in pharmacology has also been the shortest. Smoke or inject DMT and, within seconds, the ordinary world is replaced — often completely — by what people describe as another place, frequently populated by what feel like other beings. Then, in five to fifteen minutes, it is over. DMTx is the name for a set of techniques that hold that doorway open: instead of one big push of the drug, you give a smaller loading dose and then a slow, continuous drip that keeps replacing the DMT your body is frantically destroying. The result is a stable, adjustable version of the state that can last half an hour to two hours instead of a handful of minutes. That is genuinely new, and it changes what scientists can do inside the experience. Almost everything else you may have heard — that scientists have maintained a full breakthrough for six hours, that a clinic has proven the entities are real, that the whole thing is settled — is either exaggerated, unproven, or being sold to you.
A note on how to read this: every technical term is explained the first time it appears, and there is a full glossary at the end. Nothing here requires prior knowledge. If you only want the verdict, skip to "A careful scorecard" near the end. This piece walks through all of it, slowly
Part I — The molecule, and why its trip is so short
What DMT actually is
DMT stands for N,N-dimethyltryptamine. Strip away the chemistry and it is a very small, very simple molecule — small enough that it slips across the blood-brain barrier (the filter that keeps most substances out of the brain) with ease. It belongs to a family called the tryptamines, and its closest chemical relatives are two things your body makes and depends on every day: serotonin (a signalling chemical involved in mood, among a hundred other things) and melatonin (the hormone that helps run your sleep clock). DMT is, structurally, a cousin of these ordinary molecules with two small tags — two methyl groups — added on. That is the whole difference between a mood chemical and one of the most powerful consciousness-altering substances known.
DMT is not exotic in the sense of being rare. It is one of the most widely distributed psychedelics in nature, produced by a great many plants and animals — and, importantly, by mammals, including, in trace amounts, us. (We will come back to that startling fact in Part VII.)
It is most famous as the active ingredient in ayahuasca, the Amazonian brew used ceremonially for centuries. And it has been a controlled, Schedule I substance in the United States and many other countries since around 1970 — the most restrictive legal category, which has made it correspondingly hard to study.
Plain-English aside — "psychedelic." The word literally means "mind-manifesting." In practice it refers to a class of drugs — DMT, LSD, psilocybin (the compound in "magic mushrooms"), mescaline — that dramatically alter perception, thought and sense of self, usually by switching on a particular receptor in the brain (below).
What it does in the brain, briefly
A receptor is a docking port on the surface of a brain cell; when the right molecule slots into it, the cell changes its behaviour. DMT's headline effect comes from switching on one particular docking port called the 5-HT2A receptor — the same port that LSD and psilocybin use. This is the shared "master switch" of the classic psychedelics. DMT also touches several other ports (with names like 5-HT1A, 5-HT2C, sigma-1, and TAAR1), which may colour the experience, but 5-HT2A is the main event.
You do not need to remember those names. The one idea worth keeping is: DMT works by flipping a switch that is already built into your brain. It is not introducing an alien mechanism; it is over-driving an existing one.
Why a normal DMT trip is measured in minutes
Here is the crux of everything that follows.
Your body contains an enzyme — a molecular machine — called monoamine oxidase, or MAO. Its day job is to break down leftover signalling chemicals like serotonin so they do not pile up. MAO happens to treat DMT as garbage to be cleared, and it is extremely good at it. Injected or smoked DMT is torn apart and swept out of the bloodstream almost as fast as it arrives.
The numbers are stark. After an injection, DMT's level in the blood peaks within about two to three minutes and is essentially gone within twenty to thirty. Its "half-life" — the time for half of it to disappear — is only around five to seven minutes in the first, fastest phase of clearance. At any given moment, only a tiny fraction of an injected dose is even present in the blood. The experience mirrors this exactly: an almost instantaneous launch, a peak at two to three minutes, and a return to baseline before half an hour is out.
This is why smoked DMT earned the nickname "the businessman's lunch" in the 1960s — you could have the most extreme experience of your life and be back at your desk within the hour.
So how does ayahuasca last for hours? This is the elegant part. Ayahuasca is not just a DMT-containing plant. It is a combination: a DMT source plus a second plant containing MAO inhibitors (called β-carbolines — harmine, harmaline, tetrahydroharmine). An MAO inhibitor is a molecule that jams the DMT-destroying enzyme. With MAO temporarily disabled, orally swallowed DMT survives long enough to reach the brain and stays active for four to six hours. Indigenous Amazonian practice discovered, by unknown means, a two-plant pharmacological trick that Western science only reverse-engineered in the twentieth century.
Hold on to two facts, because DMTx depends on both:
- On its own, DMT is destroyed fast.
- Ayahuasca solves the "too fast" problem by blocking the destroyer (the MAO inhibitor).
DMTx solves the same problem a completely different way. It does not block the destroyer. It simply keeps replacing the DMT as fast as the body removes it. That distinction matters, and it is the heart of Part II.
Part II — The trick: how you hold the door open
Bolus versus infusion — the single most important idea
Two words do all the work here.
A bolus is a single, all-at-once dose — one push of the syringe plunger. That is how DMT has almost always been given in research: a "hit." It produces the firework — up fast, down fast.
An infusion is the opposite: the drug is fed in continuously and slowly, through a drip, over a long stretch of time.
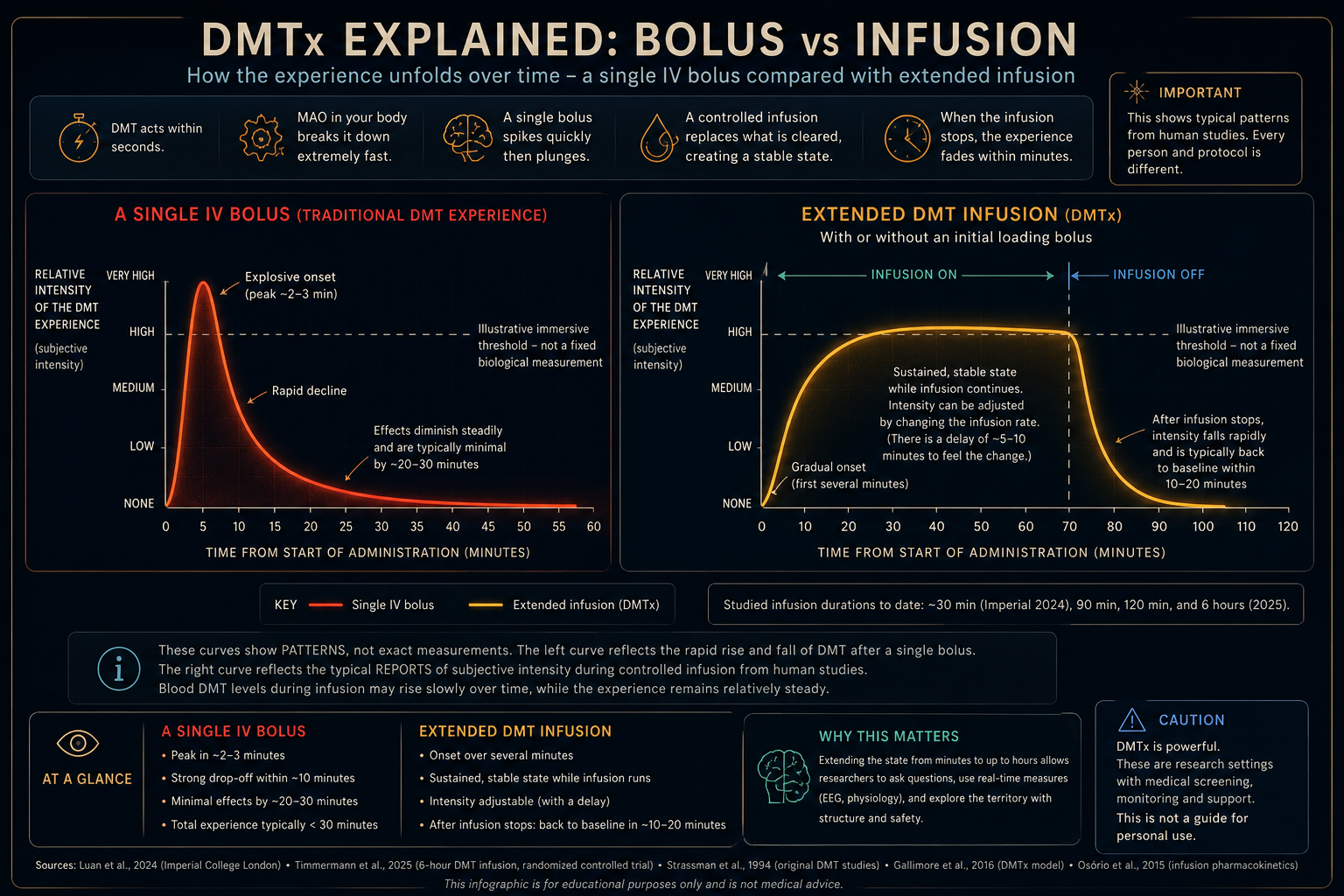
Now picture the level of DMT in the brain over time — this is exactly what the accompanying diagram shows:
- With a bolus, the line rockets up past the "breakthrough" threshold (the level at which the ordinary world gives way entirely), reaches a sharp peak, and then collapses back down as MAO clears it. A spike. Explosion, then collapse.
- With an infusion, you first give a modest loading dose to get up to the doorway quickly, and then a steady drip that puts DMT in at roughly the same rate the body is taking it out. The level rises and then holds — a plateau — for as long as you keep the drip running. Explosion, then a held plateau. When you switch the drip off, the level drops fast (because MAO is still doing its job), and the person returns to normal within minutes.
That plateau is DMTx. Everything else is engineering detail.
Why not just use an MAO inhibitor, like ayahuasca does? You could, in principle — but then you inherit ayahuasca's problems: the MAO inhibitor affects lots of other brain chemicals too, it makes the state hard to switch off quickly, and it interacts dangerously with many foods and medications. DMTx deliberately keeps DMT the only variable. Turn the drip up, the state deepens; turn it down, it lightens; turn it off, it ends — in minutes. That controllability is the entire selling point.
Borrowing a machine from the operating theatre
The founding idea of DMTx was published in 2016 by Andrew Gallimore (a neurobiologist and pharmacologist) and Rick Strassman (the psychiatrist who ran the first modern human DMT studies in the 1990s). Their paper is often misdescribed as a clinical trial. It was not. It was a modelling study — a proof of concept done with mathematics and old blood-sample data, arguing that the trick should work and showing how.
Their insight was that anaesthetists already solve this exact problem every day. During surgery, a patient must be kept at a stable depth of anaesthesia — not too light (they wake up), not too deep (dangerous). To do this, anaesthetists use target-controlled infusion (TCI): a computer-driven pump that constantly calculates how fast the body is clearing the anaesthetic and adjusts the drip to hold a chosen brain concentration steady. Gallimore and Strassman argued that DMT is almost perfectly suited to the same approach, because it ticks every box on the anaesthetist's wishlist: it dissolves in water, acts fast, wears off fast, clears quickly without building up, and — crucially — does not seem to lose its punch when repeatedly re-dosed (more on that shortly).
The recipe, in plain English
The method they proposed is sometimes abbreviated B.E.T., which stands for Bolus, Elimination, Transfer — the three things the pump has to account for. In ordinary language:
- Loading dose (the bolus). A first, quick dose to bring the level up to the doorway fast, so the person is not left waiting.
- A top-up drip that starts high and then eases off. In the first few minutes, the drug is not only being destroyed by MAO but also soaking into body tissues, so you have to feed a lot in to keep the level up. As the tissues fill and equilibrium is reached, you can throttle back to a lower, steady "maintenance" rate that simply matches ongoing destruction.
- The off switch. Stop the drip and, because MAO never stopped working, the level falls away within minutes.
Gallimore and Strassman also pointed out why an earlier attempt had gone wrong — which turns out to matter a great deal for the safety story, so we will meet it in Part III.
Part III — What actually happened when people tried it
It is one thing to model a trick on paper. Here is the real, human evidence, in order — a genuine ladder of studies, each going a little further. I have flagged what each one adds.
The starting point: the bolus studies (Strassman, 1990s)
Rick Strassman's 1994 studies were the first modern human DMT research. He gave single IV boluses and confirmed the basic time-course: effects within seconds, peak around two minutes, essentially over by thirty. These studies also produced the first careful Western documentation of the entity phenomenon (Part V) and the rating scale still used to measure the DMT state. This is the "firework" baseline everything else is compared against.
The cautionary tale: the first extended infusion (Gouzoulis-Mayfrank, 2005)
A German team ran the first genuinely extended DMT infusion — up to ninety minutes. But they set the drip rate by trial and error rather than by modelling the pharmacology, and the rate was too high: the DMT level kept climbing instead of holding steady. Three of fifteen volunteers dropped out because of distressing reactions. This is the failure Gallimore and Strassman later diagnosed: without a pharmacokinetically-informed drip rate, you don't get a plateau — you get a slow overdose. It is the single best argument for doing this carefully, and it is why later teams modelled the drip rate in advance.
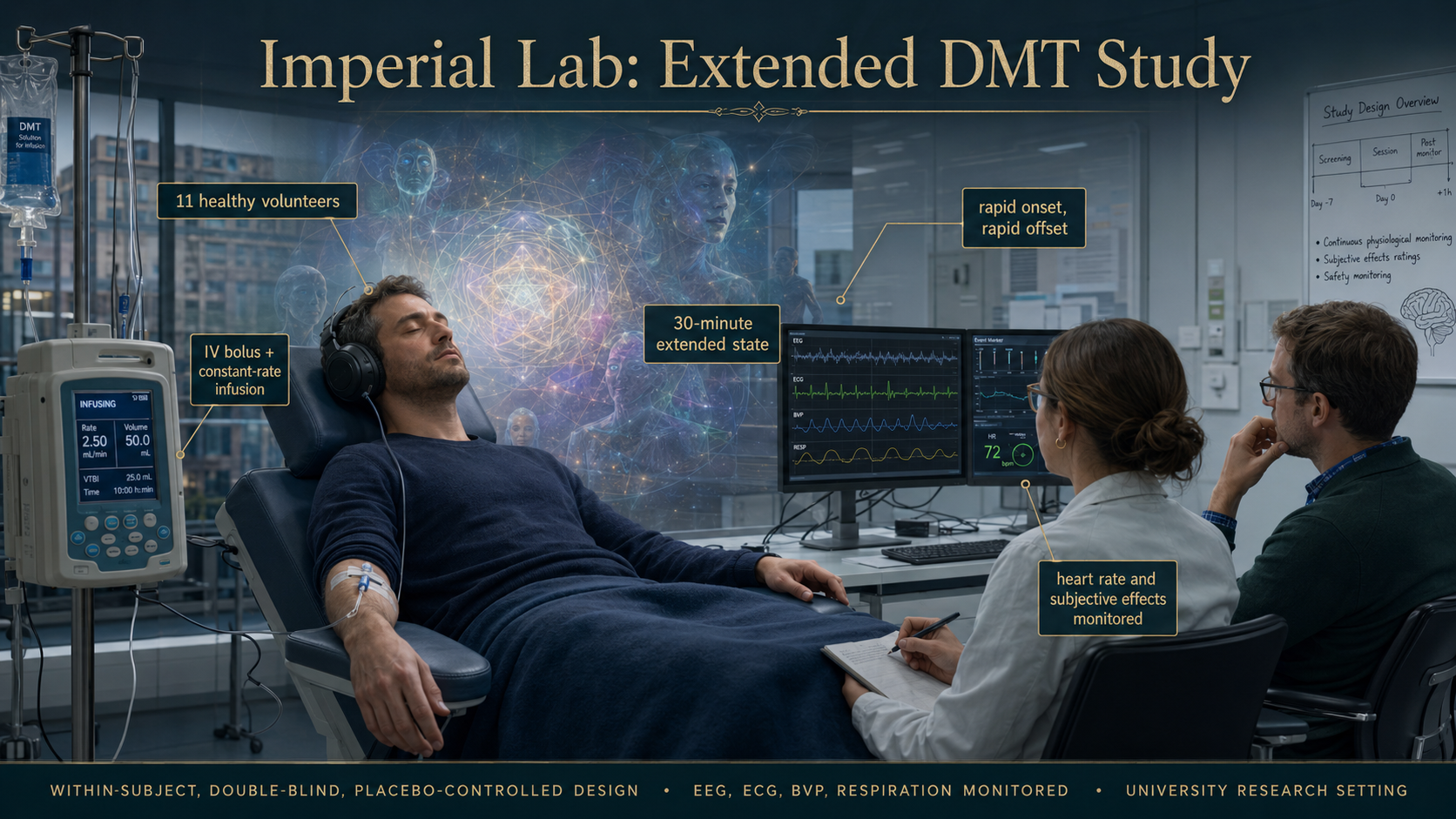
The proof it can be done cleanly: Imperial College (Luan et al., 2024)
This is the study most people mean when they say "the DMTx trial." A team at Imperial College London, with Christopher Timmermann among the authors and Lisa Luan as first author, gave eleven healthy volunteers a bolus followed by a constant-rate infusion, keeping them in the state for thirty minutes. What they found:
- It worked. Effects arrived within a minute, peaked at two, then settled into a stable plateau slightly below the peak — exactly the shape the model predicted. When the infusion stopped, everything resolved within about twenty minutes.
- It was tolerable. Anxiety stayed low. Heart rate spiked at the start but habituated — settled back toward normal — within about fifteen minutes, even while the experience continued at full strength. (One volunteer ended a higher-dose session early with anxiety and chest pain; follow-up heart tests were normal, and the team judged it psychological rather than cardiac. This is worth stating plainly rather than smoothing over: eleven carefully screened, psychedelic-experienced volunteers tolerating it is preliminary evidence of safety, not proof of safety for everyone.)
Plain-English aside — "habituation." This just means getting used to something so your reaction to it shrinks, even though the thing itself hasn't changed. Your heart "habituates" to the DMT the way your ears stop noticing a fridge hum. Keep this word; it comes back.
The current published ceiling: two hours, Basel (Erne, Vogt & Liechti, 2024)
A Swiss team at the University of Basel pushed the duration to 120 minutes — two hours — in twenty-two volunteers, and added a genuinely novel twist. Two findings stand out, and both are important enough that the hype coverage tends to miss them:
- They dropped the bolus altogether — and it was better. Rather than a loading hit plus a drip, they used a slow continuous infusion with no bolus at all. The effects climbed gradually, reached a plateau within twenty to thirty minutes, and held there for the full two hours — and this was better tolerated than a bolus, precisely because there was no violent launch to brace against. This is a real wrinkle in the original DMTx design: the loading "hit" may not be necessary, and leaving it out may be gentler.
- They let people steer. In a final session, volunteers could adjust their own dose up or down at set points to reach the intensity they wanted — the first time self-titration has been formally tested with any psychedelic. People reliably chose strong-but-manageable effects, and fear was almost absent. Because DMT switches off so fast, a change to the drip rate takes effect within five to ten minutes — you can genuinely "drive" the experience.
The Basel team also nailed down the numbers: a firm ceiling where more drug stopped producing more good effect (and only added fear), and confirmation that DMT clears in two phases — a very fast one (about six to seven minutes) that tracks the experience, and a slower tail afterwards.
The published ceiling has moved — but read the small print
You may read that DMTx has been sustained for six hours. As of 2025 that is technically true — but it is very easy to misunderstand what was actually demonstrated, and the details matter more than the headline.
In 2025, van der Heijden and colleagues at the Centre for Human Drug Research in Leiden published a randomised, double-blind, placebo-controlled trial using a thirty-second IV bolus followed by a continuous six-hour infusion in healthy volunteers. It was safe: no serious adverse events, only mild and self-limiting side effects, and no significant abnormalities in vital signs or ECG. At the highest dose, participants showed measurable changes in attention, balance and EEG activity — but the psychedelic effects were explicitly mild.
That was not a disappointing result. It was the design. The infusion reached a maximum concentration of only about 35 ng/ml — compare that with the 78–105 ng/ml the Basel team used to produce a strong psychedelic state (Part III). In other words, this study deliberately stayed at roughly a third of a breakthrough concentration. And it did so for a reason that has nothing to do with visions: the trial was funded by a pharmaceutical company (Algernon) and designed to test DMT as a possible neuroplasticity-promoting, neuroprotective treatment for stroke — where the goal is prolonged, low-level exposure to encourage the brain to rewire, not an immersive experience. The researchers were not even trying to produce the psychedelic state.
So the published literature now has two different kinds of "ceiling":
- Up to 120 minutes for a deliberately strong, adjustable psychedelic state (Basel).
- Six hours for prolonged lower-intensity administration designed to test safety, blood levels and physiological effects (van der Heijden).
"DMT has been infused for six hours" is now accurate. "Scientists have held a full DMT breakthrough open for six hours" is not. Preserving that distinction is exactly the kind of care that matters as DMTx moves from the laboratory into headlines and sales brochures.
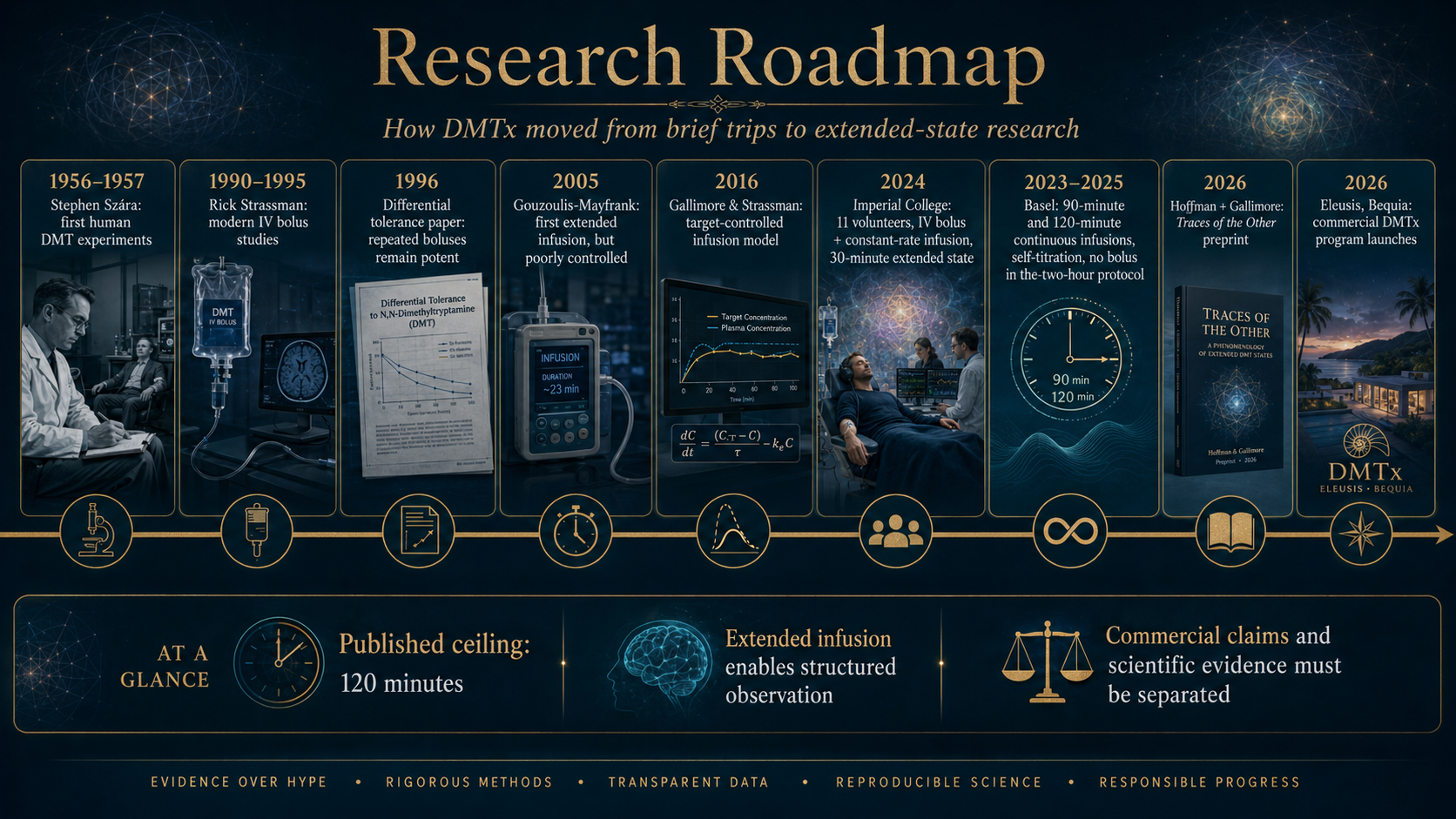
The ladder, at a glance: single bolus (~30 minutes total, Strassman in the 1990s) → first extended infusion, 90 minutes but poorly controlled (Gouzoulis-Mayfrank, 2005) → the mathematical blueprint (Gallimore & Strassman, 2016) → clean 30-minute bolus-plus-infusion (Imperial, 2024) → 90- and 120-minute continuous infusions, including self-titration without a bolus (Basel, 2023–2025) → six-hour bolus-plus-infusion at sub-psychedelic exposure, demonstrating prolonged, medically monitored administration (van der Heijden et al., 2025). The published ceiling for administration is now six hours; the published ceiling for a sustained, deliberately strong psychedelic state remains two.
A timeline of the whole story
A scannable spine — the dates that matter, in order.
- 1931 — DMT is first synthesised in the lab (Richard Manske). Nobody notices what it does.
- 1956 — Stephen Szára, a Hungarian chemist and psychiatrist, injects himself and discovers DMT is powerfully psychoactive in humans. The modern story begins.
- 1970 — DMT is placed in Schedule I, the most restrictive legal category. Research nearly halts for two decades.
- 1990–1994 — Rick Strassman runs the first modern human DMT studies (New Mexico); the landmark papers appear in 1994. This is the "firework" bolus baseline — and the first careful Western record of the entities.
- 1996 — Strassman, Qualls & Berg show that four repeated boluses produce no tolerance to the experience, while the body habituates: "differential tolerance."
- 2016 — Gallimore & Strassman publish the DMTx blueprint — a mathematical model, not a trial — borrowing target-controlled infusion from anaesthesia.
- 2019 — Dean and colleagues show the rat brain itself manufactures DMT, with levels surging after cardiac arrest.
- 2020 — Davis and colleagues publish the 2,561-person entity-encounter survey.
- 2022 — D'Souza and colleagues (Yale) find an early signal for DMT in treatment-resistant depression.
- 2023–2024 — Basel and Imperial run the first clean extended infusions: 30 minutes, then 90, then 120 — the last with no bolus and with self-steering.
- 2025 — Van der Heijden and colleagues publish a six-hour bolus-plus-infusion study in healthy volunteers, funded by a pharmaceutical company and aimed at stroke recovery. It reached only sub-psychedelic exposures (~35 ng/ml) and produced mild effects — demonstrating prolonged, medically monitored administration, not a six-hour breakthrough.
- 2026 — Eleusis opens on Bequia selling commercial DMTx; Hoffman, Gallimore & Hermansson post Traces of the Other, proposing a way to test whether the entities are real.
Part IV — The three genuinely strange findings
Extending the state didn't just make the experience longer. It exposed three things that are scientifically odd and worth understanding, because they are where DMTx stops being mere engineering and starts being interesting.
1. The mind gets used to it faster than the body clears it (acute tolerance)
Here is a genuine puzzle. During a continuous infusion, the amount of DMT in the blood keeps slowly rising after the first ten minutes or so. But the intensity of the experience does not keep rising to match — it plateaus, and can even drift down slightly. More drug, same-or-less experience. Both the Imperial and Basel teams saw this clearly.
The technical name is acute psychological tolerance — within a single session, the mind habituates to the state even as the chemical keeps accumulating. (Scientists spot it as a tell-tale mismatch between the drug-level curve and the effect curve.)
Now the beautiful contrast — and this is why the older paper Strassman, Qualls & Berg (1996) matters so much. In that study, volunteers received four separate full boluses, half an hour apart. And there was no tolerance to the psychedelic experience at all — the fourth hit was as strong as the first. This was one of the discoveries that made DMT seem unique among psychedelics, and it was part of what made DMTx seem possible in the first place.
But — and this is the elegant, easily-missed part — in that same 1996 study, the body did habituate. The stress-hormone surges (ACTH, prolactin, cortisol) and the heart-rate jump all shrank with each repeated dose, even though the subjective experience did not. Strassman called this "differential tolerance": the mind and the body were running on separate clocks.
Put the studies together and a clean picture emerges:
- Repeated, separate boluses → the experience stays fully potent (no psychological tolerance), while the body's stress response quietens down.
- One long, continuous infusion → the experience plateaus and mildly fades (some psychological tolerance appears) as the drug steadily accumulates.
So "DMT doesn't build tolerance" — a thing you will often read — turns out to be true only for one particular pattern of dosing. Change how you give it, and the picture changes. That is not a contradiction in the science; it is the science being more precise than the slogan.
2. The world is replaced, but you are still there (low ego dissolution)
With high doses of LSD or psilocybin, one of the hallmark experiences is ego dissolution — the felt boundary between "me" and "everything else" softening or vanishing, the sense of being a separate self dropping away. It is usually tied to the peak of those experiences.
DMTx produces something conspicuously different. Across the extended-state studies, people report their surroundings being completely replaced — intense imagery, immersion, encounters with apparent beings — while ego dissolution stays low. In plain terms: the world around you is swapped out for another one, but you, the observer, remain intact enough to watch it, remember it, and (in principle) report on it and run tasks inside it.
This needs one careful caveat, because it is easy to overstate. "Low ego dissolution" refers to one specific measure. Other, related measures did rise — feelings of unity, of the sacred, of transcendence, and at higher doses a "dread" of losing the self. So it is not that the self is untouched; it is that a functional, observing "you" tends to persist even while the environment is utterly transformed. And these comparisons are across different studies, not a head-to-head test of DMT against LSD in the same people — so "unlike LSD and psilocybin" is a reasonable inference, not a proven result.
Why does this matter? Because it is precisely what makes DMTx scientifically useful. If you were fully dissolved, you couldn't observe carefully, hold a question in mind, or perform a task. A preserved observer inside a fully replaced world is the thing that turns the DMT state from an unrepeatable flash into something you might actually study from the inside.
3. The beings tend to show up late
In the extended sessions, people's retrospective maps of their own experience showed something intriguing: entity encounters tended to increase in the later part of the infusion, and most clearly at higher doses — not right at the explosive onset. Immersion and visual imagery roughly tracked overall intensity, but the sense of meeting someone built over time.
Two important cautions. First, these are retrospective ratings — people reconstructing the shape of the experience afterwards, which memory distorts. The researchers were careful not to over-analyse them for this reason, and neither should we. Second, the popular claim that "entities arrive at the ten-minute mark" is too precise; the honest statement is that entity encounters rose during the later portion of the session at higher doses. (The ten-minute figure actually belongs to a different fact — that's roughly when the drug level starts climbing again during an infusion.)
Still, the direction is genuinely interesting. In a normal five-minute bolus, you would be coming down by the time this later phase arrives. Under infusion, the experience stays available long enough to develop — to move from initial visual shock toward something more like sustained encounter — rather than merely exploding and vanishing. Whether that reflects the mind settling enough to notice the beings, or the state genuinely evolving over time, is exactly the sort of question extended sessions were built to investigate.
Part V — The beings: what people actually report meeting
Any honest account of DMT has to deal with its single most consistent and most bewildering feature: at high doses, a large fraction of people report encountering what seem to be autonomous, intelligent, non-human entities. Not vague impressions — specific, interactive, apparently independent others. Rick Strassman estimated that roughly half of his high-dose volunteers reported contact with such beings. Later work puts the figure for a full "breakthrough" dose in the same range — around half.
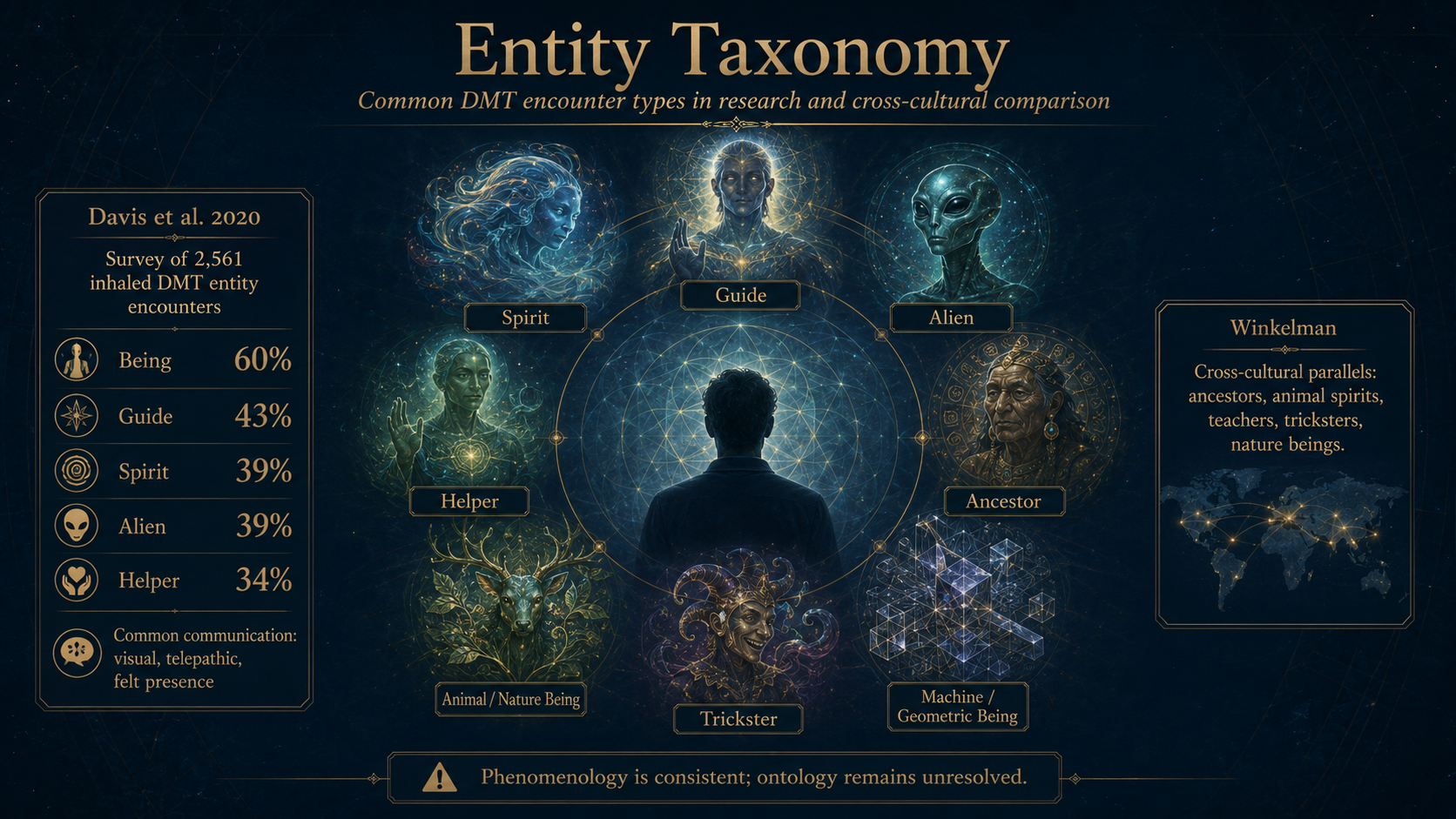
The best single source on what people report is a survey by Davis and colleagues (2020) of 2,561 people describing their most memorable DMT entity encounter. The findings are remarkably consistent:
- How the entity was perceived: overwhelmingly visual (92%) and, strikingly, "extrasensory" / telepathic (85%) — a felt, wordless exchange of meaning rather than speech.
- What people called it: the most common labels were "being" (60%), "guide" (43%), "spirit" (39%), "alien" (39%) and "helper" (34%). More specific labels (elf, angel, plant spirit, and so on) appeared at much lower rates.
- Who started it: in most cases (69%) people felt the entity initiated the encounter — it was already there, waiting, rather than summoned.
- The emotional tone: despite 41% reporting fear at some point, the dominant emotions — in the person and attributed to the entity — were love, kindness, and joy. The single most prominent emotion reported was love.
- What the entity seemed to be: most rated it as conscious (96%), intelligent (96%), benevolent (78%), and sacred (70%).
And then the part that makes this more than a curiosity — the aftermath:
- 72% believed the entity continued to exist after the encounter ended.
- 80% said the experience altered their fundamental conception of reality.
- Even after the experience, 65% rated it as "more real than" everyday waking life.
- Among people who identified as atheist beforehand, the proportion more than halved afterwards (28% → 10%); belief in a higher power, ultimate reality or universal divinity rose sharply (36% → 58%).
Researchers call this last effect "ontological shock" — a lasting jolt to a person's basic beliefs about what is real. And notably, DMT entity encounters closely resemble non-drug reports from utterly different contexts: religious visions, near-death experiences, and even alien-abduction accounts show overlapping features. Whatever is happening, it is tapping into something deep and cross-cultural in human experience.
▨ Why do the same beings keep appearing?
For decades the anthropologist Michael Winkelman has catalogued strikingly similar entity encounters across wildly separate traditions — Amazonian ayahuasca, Siberian and Mongolian shamanism, African initiatory religions, Native American ceremony — and across non-drug states too: dreams, sleep paralysis, and near-death experiences. His argument is not that this proves spirits are real. It is almost the reverse, and more interesting: that something in the shared architecture of the human mind reliably produces the same categories of being — the guide, the guardian, the trickster, the healer, the teacher — whoever you are and wherever you live.
That quietly reframes the whole "are they real?" debate. Because whichever side you favour — the brain generates them, or the brain perceives them — the deeper puzzle is the consistency. Why these beings and not others? Why the same recurring cast, across every culture that has ever looked? Any complete theory of the DMT state has to explain not merely that people meet entities, but why humanity keeps meeting the same ones.
None of this, it must be said clearly, tells us whether the beings are real in any external sense. It tells us that the experience of meeting them is vivid, consistent, emotionally profound, and life-altering. That is the phenomenon to be explained — not the answer to it.
Part VI — The big question: are the entities "real"?
This is where DMTx collides with the deepest question in the whole field, and where you should hold on to your wallet and your credulity, because it is also where the marketing gets loudest.
There are, broadly, two hypotheses.
Hypothesis A — the entities are internally generated. They are produced by your own brain: by its social machinery (the same circuitry that models other minds), its agency-detection systems (evolved to spot predators and allies, and prone to firing even when nothing is there), its visual and emotional systems, all thrown into an extraordinary state. On this view the beings feel utterly real for the same reason dream characters feel real while you dream — because your brain is very good at generating convincing others. This is the mainstream neuroscientific default, and it is the more conservative position: it requires no new assumptions about the universe.
Hypothesis B — the entities are, at least sometimes, perceptions of something not generated solely by you. This is the radical option, and it has just acquired its most serious formulation.
Conscious realism, in plain English
The cognitive scientist Donald Hoffman has spent years arguing a counter-intuitive idea called conscious realism. The easiest way in is his own metaphor: your perception of the world is like a computer desktop. The icons on a desktop — little folders and files — are useful, but they are not what is really going on inside the machine (which is voltages and logic gates you never see). Hoffman argues that space, time, and physical objects are like those icons: a species-specific interface evolved to keep us alive, not a truthful picture of ultimate reality. He backs this with a mathematical result he calls "Fitness Beats Truth": evolution, he argues, actively favours perceptions that are useful over perceptions that are accurate, because the two usually come apart.
If that is right, then what is "really" out there is not matter in space but — in his framework — a vast network of interacting conscious agents, of which our ordinary interface shows us only a thin sliver. The rest is filtered out, not because it isn't there, but because seeing it never helped our ancestors survive.
The provocative move is obvious once you see it: what if DMT alters the interface itself — nudges the "desktop" so that agents normally filtered out briefly leave a mark on experience? On this view the entities would be neither hallucinations nor spirits in the traditional sense, but traces of parts of reality our everyday perception is built to ignore.
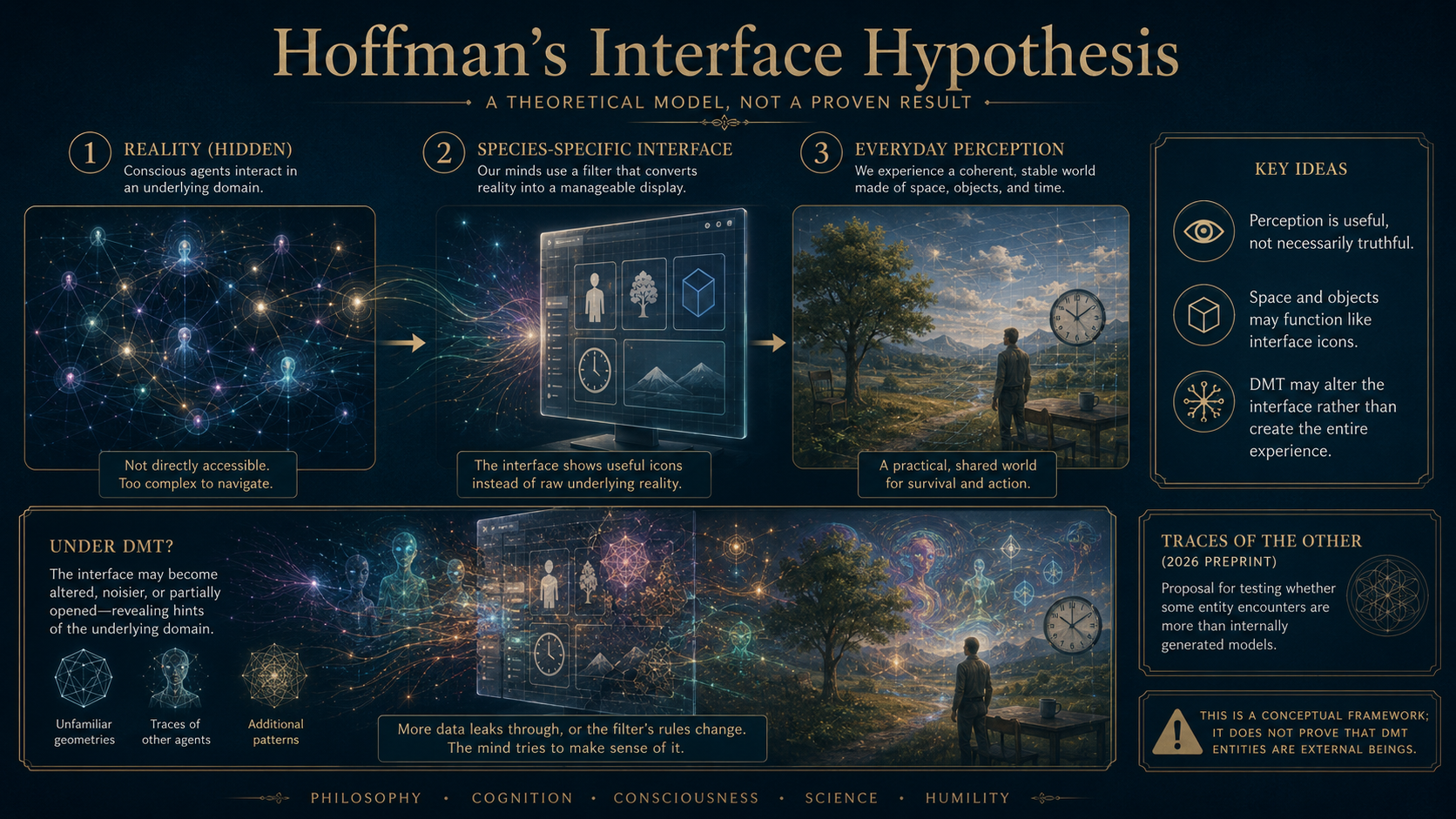
"Traces of the Other" (2026) — what it is, and what it is not
In May 2026, Hoffman, Gallimore, and the mathematician Niffe Hermansson posted a preprint titled Traces of the Other – Are DMT Entities Real?, laying out this framework in full mathematical dress. It has drawn enormous attention, so it is worth being extremely precise about what it actually is:
- It is a preprint — posted online, not yet peer-reviewed.
- It is theoretical. By the authors' own statement, it reports no experiments and no data. It is a proposal.
- Most importantly: it explicitly keeps the "hallucination" explanation as the default. Its actual claim is modest and, frankly, reasonable — that the external-agent hypothesis has been dismissed rather than tested, and that it can be reformulated so that it could, in principle, fail a test. That is a legitimate scientific move. It is a long way from "scientists have shown the entities are real," which is how it is sometimes reported.
The two organisations involved divide the labour: Noonautics (Gallimore's non-profit) would supply the extended-state DMTx protocol to send trained observers into the state; the Trace Institute (Hoffman's) supplies the mathematics. The plan is to have skilled observers make careful, structured observations inside long DMT sessions and derive predictions that could distinguish Hypothesis A from Hypothesis B.
How would you ever test such a thing?
This is the genuinely hard part, and it is worth understanding why. Simply asking people "did it feel real?" settles nothing — DMT entities already feel more real than reality. The felt-realness is the thing being explained, not evidence for either side.
A real test needs observations that would come out differently depending on which hypothesis is true. The kinds of experiments proposed (by these authors and others over the years) include:
- Hidden-target tasks. A computer randomly picks a symbol or number after the person is already in the state; nobody present knows it. The person asks the entity for the answer. Getting it right, repeatedly, above chance, would be very hard to explain by "your own brain made it up."
- Separated-participant tests. Two people, in isolated rooms, asked to reach the "same place" or a shared target. Mere similar imagery wouldn't count — you'd need precise, pre-specified correspondence.
- Repeat-visit mapping. Can a person return to the "same" location or entity across sessions, with independent judges scoring the consistency against criteria fixed in advance?
- Perturbation. Change some hidden external variable and see whether features of the reported world track it in a predicted way.
The catch that won't go away
Even a perfectly repeatable, richly detailed entity encounter would not, by itself, prove the beings are external — because humans share a brain design. Shared wiring can produce shared experiences with no external cause: migraine sufferers who have never met report the same geometric "fortification" patterns; dreamers everywhere meet convincing people their own brains invented. This is the problem of underdetermination — the same evidence fitting more than one explanation.
But — and this cuts both ways — calling something a "hallucination" names its presumed origin without actually explaining it. Why are DMT worlds so densely populated? Why do the beings seem autonomous? Why do technological and "hyperdimensional" motifs recur? Why can the sense of reality exceed waking life? Neuroscience owes real answers here, and does not yet have them. The most defensible position today is the conservative one — internally generated — held with genuine humility about how much remains unexplained. And the one thing Gallimore and Hoffman are clearly right about, whatever you make of their metaphysics, is the methodological point: an idea that can be tested and fail is better than one argued forever through anecdote.
The other side of the table — the naturalists' reply
It would be easy to leave Part VI thinking the Hoffman–Gallimore view is the only game in town. It is not, and it is ARDMT's job to say so plainly. The large majority of neuroscientists and philosophers of mind hold that DMT entities are generated by the brain — and they are not merely asserting it. They have detailed, well-developed frameworks that account for the phenomenology without invoking anything outside the skull. A fair reader should weigh these before being swept away.
The "controlled hallucination" view (Anil Seth and the predictive-processing tradition). On this now-mainstream account, ordinary perception is always a kind of controlled hallucination: your brain never sees the world directly, it constantly generates a best-guess model and corrects it against incoming signals. What you experience is the model, not the raw world. Psychedelics, on this view, don't open a door to elsewhere — they loosen the brain's grip on its own predictions, so the model runs unusually free. The entities are what an unconstrained world-model produces once its normal reality-checks are turned down. No new physics or metaphysics required.
The free-energy / active-inference tradition (Karl Friston and colleagues). A more mathematical cousin of the above: the brain is cast as a prediction machine forever trying to minimise "surprise," and its deep, high-level assumptions about reality are called priors. Which leads directly to —
The entropic brain and REBUS (Robin Carhart-Harris). Here is the delicious irony: Carhart-Harris is one of the authors of the very Imperial extended-DMT study at the centre of this piece. His model, developed with Friston, is called REBUS — "RElaxed Beliefs Under pSychedelics." The idea is that psychedelics relax the brain's highest-level priors, letting lower-level activity bubble up unchecked and raising the "entropy" (roughly, the richness and disorder) of brain activity. The DMT world, on this account, is precisely what you get when the brain's ordinary constraints are released: vivid, autonomous-seeming, more-real-than-real — and entirely home-made. In other words, one of the people who built the tool that makes Hoffman's experiments possible holds a thoroughly naturalistic view of what those experiments will find.
The hard sceptic (David Nichols). Nichols, an eminent medicinal chemist, has spent years pushing back on romantic readings of DMT — arguing, for instance, that the "the pineal gland floods you with DMT" story is myth, and that endogenous DMT levels are almost certainly far too low to do anything mystical. He is the reliable cold shower, and the field is healthier for him.
Even the adventurous camp disagrees with itself. This is not a tidy "Hoffman versus the mainstream." Andrés Gómez-Emilsson, at the Qualia Research Institute, offers a different non-standard account — that DMT drives experience into a regime of such extreme energy that the very geometry of perceived space reorganises into hyperbolic, higher-dimensional forms. Whether that supports Hoffman's conscious agents or merely rhymes with them is unresolved. The point is that "the entities are more than hallucinations" is not one idea but several competing ones.
A fair bottom line: as of this writing, no formal, peer-reviewed rebuttal of Traces of the Other has appeared — the preprint is only weeks old and, being a proposal rather than a result, there is as yet nothing empirical to rebut. But the frameworks above are how mainstream neuroscience already explains everything in Part V without ever leaving the head. The honest state of play is not "Hoffman is winning." It is this: a bold, testable proposal has been made, and a large, well-armed naturalist consensus is waiting to see whether any experiment can trouble it.
Part VII — Is it already inside us?
A fact that unsettles people the first time they hear it: your own body makes DMT. It is one of the very few psychedelics produced endogenously — that is, internally — by mammals, including humans. This has fuelled decades of romantic speculation. Here is the careful version.
The manufacturing pathway is known: from the dietary amino acid tryptophan, the body makes tryptamine, and then an enzyme called INMT (indolethylamine-N-methyltransferase) adds the two methyl tags that turn it into DMT. That much is solid.
The strongest recent evidence comes from Dean and colleagues (2019), who showed that the rat brain contains the full machinery to make DMT (the necessary enzymes sitting together in the right cells), and detected DMT in the living rat cortex at levels comparable to familiar signalling chemicals like serotonin. Most evocatively, they found DMT levels surged in the brain after cardiac arrest — which is catnip for anyone interested in near-death experiences.
Now the discipline. This is precisely the kind of finding that gets over-read, so:
- The "comparable to serotonin" claim is contested. A pointed critique (led by David Nichols, a very senior figure in the field) argues the concentrations are still far too low to produce a psychedelic effect under normal conditions, and that "we can make it" is not the same as "it does something."
- We genuinely do not know what endogenous DMT is for. Leading guesses involve protection of brain cells under stress (via that sigma-1 receptor mentioned earlier) or a role in early development — not necessarily anything to do with visions at all.
- The popular story that "your brain floods you with DMT as you die" is, at present, not established. The cardiac-arrest surge in rats is real and fascinating; the leap to explaining human near-death experiences is speculation, not fact.
The honest summary: DMT is unmistakably present in us, its purpose is unknown, and every strong claim about that purpose currently outruns the evidence. Which is itself a good reason to keep studying it — and a good reason not to believe the confident stories.
Part VIII — The medical angle
Set the metaphysics aside entirely, and there is a sober, practical reason for interest in DMTx: depression.
The clearest human hint so far comes from D'Souza and colleagues (2022) at Yale, who gave IV DMT to a small group including seven people with treatment-resistant depression — people who had failed multiple prior treatments, ill for decades on average. The day after the higher dose, their depression scores dropped meaningfully (a medium-to-large effect). Two details make this genuinely interesting for ARDMT's purposes:
- It was done in a plain hospital room — no art, no curated music, minimal psychotherapy — and still showed an effect. This speaks to a live debate in the field about how much of psychedelic therapy's benefit depends on elaborate "set and setting" versus the drug itself.
- DMT showed low signs of abuse potential — after the session, people were, if anything, less keen to repeat it, and valued it at a token amount.
This was a small, open-label, early-stage study — a hint, not a verdict. But it points to why the extended state is attractive for medicine specifically. With DMTx you could, in principle, tune a therapeutic session in real time: ease someone in gently, deepen the state to do difficult work, create calmer "rest periods," then bring them down — all within a session that lasts a manageable half-hour to two hours rather than the six to twelve hours of psilocybin or LSD. Because DMT switches off within minutes of stopping the drip, it is, in one specific sense, more controllable — and therefore potentially safer and cheaper to deliver — than any other classic psychedelic. That controllability, not mysticism, is the strongest practical case for the whole enterprise.
Part IX — The Bequia question: where science meets salesmanship
Everything above is research. This section is commerce, and it is where a sceptical eye earns its keep.
In early 2026, a private operation called Eleusis announced its debut on the island of Bequia, in Saint Vincent and the Grenadines, describing itself as "the world's first legal luxury psychedelic immersion" built around DMTx protocols. It is a residential, high-end, invitation-style programme with medical staff, and it lists Christopher Timmermann — one of the genuine Imperial researchers — as its research director.
There is nothing inherently wrong with a legal, medically-supervised centre. But several things deserve a clear, unsentimental eye, and this is exactly the sort of place where ARDMT's job is to separate what is demonstrated from what is asserted:
On the science being claimed. Eleusis's own materials describe holding a "breakthrough" state for 30 to 60 minutes — which is squarely within what the published research supports, and notably shorter than the "two-hour" figure that floats around in coverage. So far, so reasonable. But the same materials also make striking claims — "sustained reductions" in treatment-resistant depression and PTSD, a "30 percent rise in executive function" at 60 days — attributed to "pilot cohorts" with no published data behind them. Those are marketing numbers, not findings. Testimonials and glossy outcome figures are not the same thing as peer-reviewed evidence, and the distinction should be kept bright.
On "legal" and "licensed." These are the operation's own descriptions. The interesting question — and one worth asking precisely rather than waving through — is: legal under exactly what instrument? A specific national licence? A research authorisation? A gap in local law? "World's first legal" is a marketing phrase until an actual legal basis is identified and can be examined. This matters because the word "legal" is doing enormous reassurance-work for a prospective participant, and reassurance is precisely what should be evidence-backed.
On the research-versus-retreat boundary. Describing a paid immersion as a "research immersion" blurs a line that ethics committees exist to keep sharp. In real research, participants are volunteers in an ethically-approved protocol with independent oversight; they are not customers. When guests pay for an experience and are described as contributing to research, it is fair to ask who owns the data, who approved the protocol, and whether marketing and science are being allowed to launder each other's credibility. (It is worth noting that public criticism along exactly these lines already exists.)
None of this is to prejudge Eleusis specifically. It is to model the questions any reader should bring to any commercial DMTx offering — because the gap between "a real technique with real published support" and "a luxury product wrapped in that technique's prestige" is precisely where people get misled.
A careful scorecard
Pulling the whole thing together — what is solid, what is shaky, and what is genuinely new:
Solid.
- A normal DMT experience really is over in minutes, because the enzyme MAO destroys it almost as fast as it arrives.
- DMTx — a loading dose (or none) plus a continuous drip — really can hold the state stable for up to two hours, safely and tolerably, in screened healthy volunteers.
- Continuous infusion without a bolus appears better tolerated than the original bolus-based design (Basel).
- The state shows acute psychological tolerance during a long infusion (effects plateau as drug levels keep rising), while repeated separate boluses show no such tolerance to the experience — a real, precise, and initially confusing pair of facts that fit together once you separate "the mind" from "the body" and "one long dose" from "several separate ones."
- Entity encounters are common (around half of breakthrough experiences), consistent, emotionally profound, and frequently life-altering. The experience is beyond dispute.
- The body makes DMT; what for is unknown.
- There is an early, real hint that DMT may help treatment-resistant depression.
Shaky or overstated.
- "Six-hour breakthrough trips": unsupported. A six-hour infusion has now been published, but it was deliberately kept at roughly a third of a breakthrough concentration (~35 ng/ml) for a stroke-neuroplasticity study, and produced only mild effects. The longest published deliberately-strong, sustained psychedelic sessions remain two hours.
- "Entities appear at ten minutes": too precise; they rise later in the session at higher doses, per retrospective (memory-based) ratings.
- "Endogenous DMT explains near-death experiences" / "is at functional levels in the brain": contested and, at best, unproven.
- Commercial claims of specific therapeutic outcomes ("30% cognitive improvement," etc.): marketing, not evidence.
- "Scientists have shown DMT entities are real": false. What exists is a theoretical, un-peer-reviewed proposal to make the question testable — which still treats "hallucination" as the default.
Genuinely new — and the real story. The headline is not that anyone has proven anything about the nature of the beings. It is quieter and more important: for the first time, extended infusion turns the DMT state from an almost un-observable flash into a stable, adjustable, steerable environment — one a person can remain inside, with a functioning observing self, long enough to look around, hold a question, and perform a task. That is what makes better science newly possible. It is also what makes it newly possible to build an attractive commercial mythology on top of findings that remain early. Both things are true at once, and telling them apart is the whole game.
Coda — what actually changed
For seventy years DMT has been one of science's sharpest paradoxes: quite possibly the most extraordinary experience a human nervous system can have, and almost impossible to study — because it vanishes before careful observation can begin. You cannot map a country you are only ever flung through at speed.
Extended-state DMT changes that, and this is the thing to hold on to when the metaphysics gets loud. Whether the worlds people enter are spun entirely from their own neurons, or are glimpses of something our ordinary senses are built to screen out, or are something our present categories simply fail to capture — the decisive shift is methodological, not metaphysical. For the first time, a person can stay inside the experience long enough, stably enough, and clear-headed enough to ask a structured question and watch what happens, rather than stagger out clutching a fading memory.
That does not answer the mystery. It does something rarer: it turns an unanswerable mystery into an investigable one. The door that used to slam shut in five minutes can now be held open — and what waits on the other side is, at last, a question that experiments, and not only stories, might begin to settle.
Glossary (the A-to-Z)
5-HT2A receptor — the main "docking port" in the brain that DMT (and LSD, and psilocybin) switches on to produce its effects.
Acute tolerance — getting used to a drug's effect within a single session, so the same amount does less. DMT shows this during a long infusion, but not across repeated separate injections.
Ayahuasca — an Amazonian brew combining a DMT-containing plant with a second plant that blocks the DMT-destroying enzyme (MAO), so the DMT lasts for hours when drunk.
Blood-brain barrier — the biological filter that keeps most substances out of the brain. DMT crosses it easily.
Bolus — a single, all-at-once dose. The "firework." Contrast with infusion.
Breakthrough — the point at which a high enough dose replaces the ordinary world entirely with the DMT "space."
Conscious realism — Donald Hoffman's theory that physical reality (space, time, objects) is a useful "interface," like desktop icons, rather than a true picture of what's really there.
DMT — N,N-dimethyltryptamine. A small, fast-acting, extremely powerful psychedelic molecule, chemically related to serotonin and melatonin, found throughout nature and made in trace amounts by the human body.
DMTx — extended-state DMT: techniques (loading dose and/or continuous infusion) that hold the DMT experience stable for far longer than the usual few minutes.
Ego dissolution — the felt dropping-away of the boundary between self and world. Prominent with LSD/psilocybin; conspicuously low in DMTx (the world is replaced but "you" remain to watch).
Endogenous — produced inside the body. Human beings make DMT endogenously.
Entity encounter — the experience, reported by roughly half of breakthrough users, of meeting apparently autonomous, intelligent, non-human beings.
Habituation — getting used to something so your reaction shrinks, even though the thing hasn't changed.
Half-life — the time for half of a drug to be cleared from the body. DMT's is very short (minutes).
Infusion — feeding a drug in slowly and continuously through a drip, rather than all at once. The basis of DMTx.
MAO (monoamine oxidase) — the enzyme that destroys DMT very rapidly. The reason a normal DMT experience is so short.
MAO inhibitor — a substance that jams MAO. Ayahuasca uses one; DMTx deliberately does not.
Ontological shock — a lasting jolt to a person's basic beliefs about what is real, frequently reported after DMT entity encounters.
Pharmacokinetics — the study of how a drug moves through the body over time: how fast it's absorbed, distributed, and cleared. The maths behind the DMTx drip rate.
Preprint — a scientific paper posted publicly before peer review. Not yet vetted by independent experts.
Psychedelic — "mind-manifesting"; a class of drugs (DMT, LSD, psilocybin, mescaline) that profoundly alter perception, thought, and sense of self.
Receptor — a docking port on a brain cell that changes the cell's behaviour when the right molecule slots in.
Retrospective rating — describing an experience after it's over, from memory (and therefore vulnerable to distortion).
Serotonin — an everyday signalling chemical in the brain, chemically a close relative of DMT.
Target-controlled infusion (TCI) — a computer-driven pump system, borrowed from anaesthesia, that holds a chosen drug level steady by constantly adjusting the drip. The engineering heart of DMTx.
Tolerance — needing more of a drug for the same effect, after repeated use. DMT's tolerance behaviour is unusual and depends on how it's given.
Tryptamine — the chemical family DMT belongs to, which also includes serotonin and melatonin.
Underdetermination — the situation where the same evidence is consistent with more than one explanation, so it can't decide between them. The core difficulty in the "are the entities real?" question.
Sources and further reading
The founding concept
- Gallimore, A. R. & Strassman, R. J. (2016). A model for the application of target-controlled intravenous infusion for a prolonged immersive DMT psychedelic experience. Frontiers in Pharmacology, 7, 211.
The human extended-state studies (the ladder)
- Gouzoulis-Mayfrank, E., et al. (2005). Psychological effects of (S)-ketamine and N,N-dimethyltryptamine (DMT). Pharmacopsychiatry, 38, 301–311. (First extended infusion; the cautionary precedent.)
- Luan, L. X., et al. (2024). Psychological and physiological effects of extended DMT. Journal of Psychopharmacology, 38(1), 56–67. (Imperial College; 30-minute bolus-plus-infusion.)
- Vogt, S. B., et al. (2023). Acute effects of intravenous DMT in a randomized placebo-controlled study in healthy participants. Translational Psychiatry, 13, 172. (Basel; 90-minute infusions.)
- Erne, L., Vogt, S. B., … Liechti, M. E. (2024/2025). Acute dose-dependent effects and self-guided titration of continuous N,N-dimethyltryptamine infusions. Neuropsychopharmacology, 50(6), 1008–1016. (Basel; the 120-minute study, no bolus, self-titration.)
- van der Heijden, K. V., Zuiker, R. G. J. A., Otto, M. E., Bryan, C. S., Stewart, N., Stillwell, C., De Kam, M. L., van Leuken, M. B., van Gerven, J. M. A. & Jacobs, G. E. (2025). Safety, Pharmacokinetics, and Pharmacodynamics of a 6-h N,N-Dimethyltryptamine (DMT) Infusion in Healthy Volunteers: A Randomized, Double-Blind, Placebo-Controlled Trial. Clinical and Translational Science, 18(5), e70234. (Funded by Algernon Pharmaceuticals; designed as a stroke-neuroplasticity study, not a psychedelic one.)
Tolerance and the bolus baseline
- Strassman, R. J., Qualls, C. R. & Berg, L. M. (1996). Differential tolerance to biological and subjective effects of four closely spaced doses of N,N-dimethyltryptamine in humans. Biological Psychiatry, 39, 784–795.
- Strassman, R. J. & Qualls, C. R. (1994). Dose-response study of N,N-dimethyltryptamine in humans, parts I & II. Archives of General Psychiatry, 51, 85–108.
The entities
- Davis, A. K., et al. (2020). Survey of entity encounter experiences occasioned by inhaled N,N-dimethyltryptamine. Journal of Psychopharmacology, 34(9), 1008–1020.
- Winkelman, M. J. (2018). An ontology of psychedelic entity experiences in evolutionary psychology and neurophenomenology. Journal of Psychedelic Studies, 2, 1–19.
The "are they real?" question
- Gallimore, A. R., Hermansson, N. & Hoffman, D. D. (2026). Traces of the Other – Are DMT Entities Real? DMT Phenomenology in the Framework of Conscious Realism. PsyArXiv preprint (awaiting peer review). DOI: 10.31234/osf.io/8qvgy_v2.
- Hoffman, D. D. (2019). The Case Against Reality. (Book-length statement of conscious realism and Fitness-Beats-Truth.)
Endogenous DMT
- Barker, S. A. (2018). N,N-Dimethyltryptamine (DMT), an endogenous hallucinogen. Frontiers in Neuroscience, 12, 536.
- Dean, J. G., et al. (2019). Biosynthesis and extracellular concentrations of N,N-dimethyltryptamine (DMT) in mammalian brain. Scientific Reports, 9, 9333.
- Nichols, D. E. (2018). N,N-dimethyltryptamine and the pineal gland: separating fact from myth. Journal of Psychopharmacology, 32, 30–36. (The sceptical counterweight.)
Medicine
- D'Souza, D. C., et al. (2022). Exploratory study of the dose-related safety, tolerability, and efficacy of dimethyltryptamine (DMT) in healthy volunteers and major depressive disorder. Neuropsychopharmacology, 47, 1854–1862.
Background pharmacology
- Cameron, L. P. & Olson, D. E. (2018). Dark Classics in Chemical Neuroscience: N,N-Dimethyltryptamine (DMT). ACS Chemical Neuroscience, 9, 2344–2357.
The commercial edge (read critically)
- Eleusis promotional materials and press releases (2026), Bequia, Saint Vincent and the Grenadines. (Marketing, not peer-reviewed evidence — cited here as primary source material for what is being claimed, not as findings.)