Research
DMT vs Ketamine: Equal on Depression, DMT Wins on Anxiety
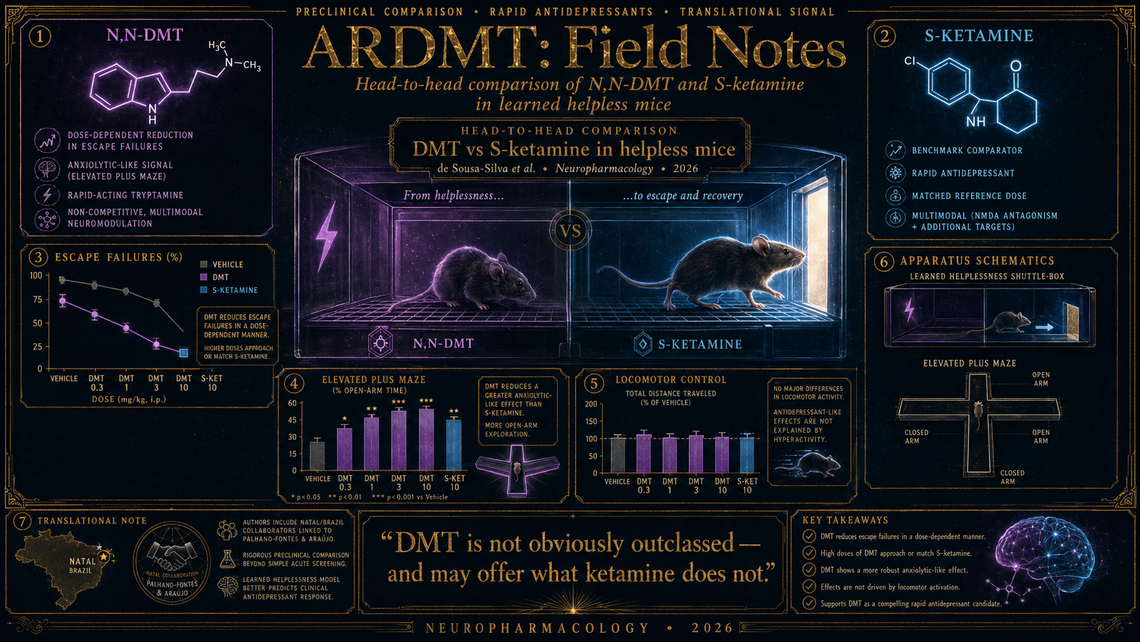
A Brazilian–Natal collaboration led by de Sousa-Silva and colleagues has done something that sounds deceptively simple but has, until now, been curiously absent from the literature: they sat DMT and S-ketamine side by side in the same behavioural paradigm, using the same animals, at the same timepoints, and asked which compound does what, and at what dose (PMID 41881297). The paper, published in Neuropharmacology and indexed for MEDLINE as of April, uses a learned helplessness model in mice — still one of the more demanding preclinical depression assays, in that it requires animals to first acquire a helpless phenotype before treatment, rather than simply measuring a naïve mouse's willingness to swim.
Design and methods
The model itself will be familiar to anyone who has spent time in a behavioural pharmacology laboratory: inescapable foot shock over several sessions produces a subset of mice that subsequently fail to escape even when escape is available. These "helpless" animals — and the authors appear to have been reasonably stringent in their selection criteria — then received intraperitoneal injections of DMT across a dose range, S-ketamine at a standard reference dose, or vehicle, before being tested in the escape paradigm and in an elevated plus maze to capture both depressive-like and anxiety-like dimensions. The study also tracked locomotor activity, which is essential housekeeping: if your antidepressant merely makes the mouse more motile, you have not demonstrated an antidepressant effect so much as a stimulant one.
The inclusion of both the escape-failure test and the elevated plus maze in the same cohort is a genuine strength. Depression and anxiety are notoriously comorbid in the clinic, and while S-ketamine has robust data for the former, its anxiolytic credentials remain debatable. Comparing the two compounds across both behavioural domains within one protocol gives us something cleaner than stitching together results from separate laboratories with different strains, handling practices, and lighting conditions.
Key findings
DMT produced dose-dependent reductions in escape failures — the core readout of helplessness — with the higher doses approaching or matching the effect size of S-ketamine. That in itself is not a shock; DMT has shown antidepressant-like activity in forced swim and tail suspension tests before. What is more interesting is the anxiety arm: DMT increased open-arm exploration in the elevated plus maze, suggesting an anxiolytic effect that the S-ketamine comparator did not reliably produce at the dose tested. If the anxiolytic signal holds up, this would be a meaningful differentiator in a clinical landscape where ketamine's acute anxiogenic potential is a real practical concern — dissociation, after all, is not always a comfortable experience.
Locomotor activity did not appear to account for the behavioural improvements, which is reassuring, though one always wishes for a few more control conditions (an open field at a later timepoint, perhaps, or a non-serotonergic comparator) to be truly confident that what looks like reduced despair is not simply altered exploration.
What is well supported and what is not
The head-to-head design, the use of a validated helplessness model rather than a simpler acute screening test, and the dual-domain assessment all mark this as a more rigorous preclinical comparison than most of what has been published. The dose–response curve for DMT gives useful information for anyone planning translational work. And the authorship team — which includes Palhano-Fontes and Araújo, who ran the landmark treatment-resistant depression trial with ayahuasca — brings a certain translational seriousness to the enterprise.
That said, this is a single study in male mice (one assumes male, as is regrettably still the default in much of this literature), using a single route of administration, at acute timepoints. We do not know whether the anxiolytic effect persists beyond a few hours. We do not know the receptor pharmacology driving it — is this a 5-HT2A story, a sigma-1 contribution, or something else entirely? And the learned helplessness model, for all its virtues, has a patchy record of predicting clinical efficacy in compounds that act outside conventional monoaminergic pathways. It told us very little, for instance, about the timeline of ketamine's effects in humans. One would want to see chronic dosing schedules, female cohorts, and ideally a mechanistic arm involving selective antagonists before drawing strong translational conclusions.
Still, as a first clean comparison with the current clinical gold standard, it does what it needed to do: it places DMT in the same frame and finds that the molecule is not obviously outclassed, and may in fact offer something ketamine does not.
Also worth a glance
A team using awake-rat fMRI has mapped dose- and sex-dependent effects of 5-MeO-DMT on whole-brain connectivity, revealing striking sexual dimorphisms in thalamo-cortical coupling that should give pause to anyone designing single-sex preclinical tryptamine studies (PMID 41796937). Separately, a preprint on 2-halogenated tryptamine structure–activity relationships explores how strategic halogen placement shifts receptor selectivity profiles across the serotonergic landscape — pharmacological locksmithing of the kind that may eventually let us tune tryptamine therapeutics away from hallucinogenic liability (PMID 42079221; preprint, not yet peer-reviewed).
Marginalia
It is quietly remarkable that the compound Szára first injected into his own arm in a Budapest laboratory in 1956 is now being benchmarked against a drug that earned Johnson & Johnson billions. The distance between self-experiment and systematic preclinical comparison is, in one sense, enormous; in another, the field has been extraordinarily slow to walk it. One trusts the next seventy years will be more briskly paced.