ARDMT Field Notes
DMT for Stroke: Exeter Knockout Data Challenges Sigma-1 Story
There is a particular kind of experimental result that makes you put your tea down. Not the kind that confirms a hypothesis — those are gratifying but rarely instructive — but the kind that does something almost impolite: it removes the thing you thought was doing the work, and the work gets done better. That is, in essence, what a group at the University of Exeter appears to have found with DMT and spreading depolarisations, and it has implications that ripple outward rather forcefully through the mechanistic assumptions underpinning the current DMT-for-stroke translational pipeline.
The finding, and why it is awkward
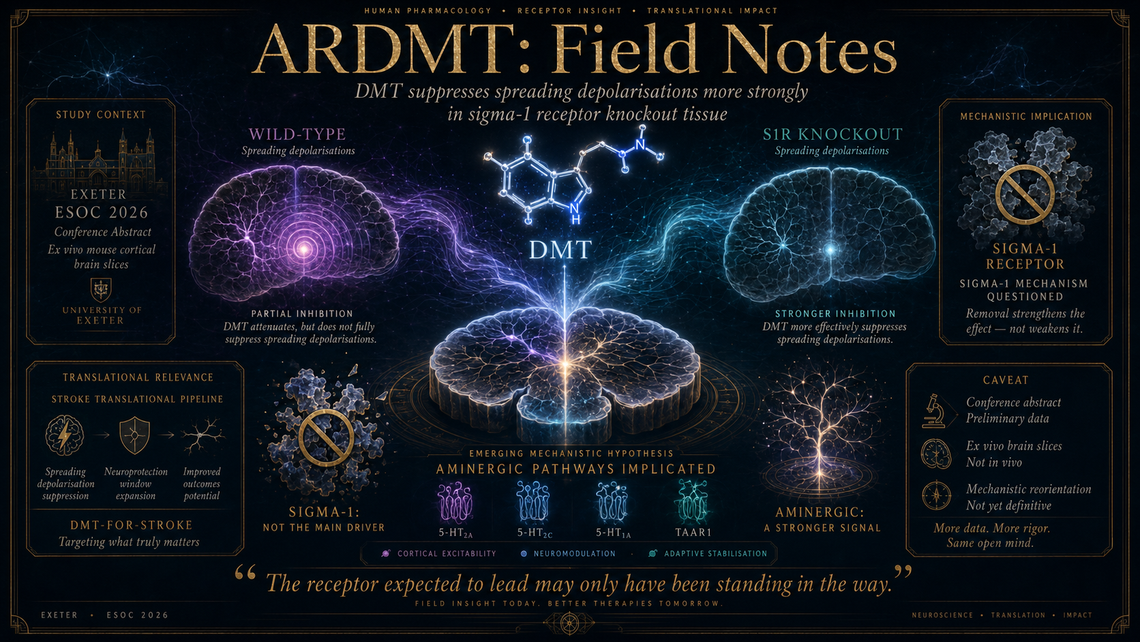
The abstract in question (DOI 10.1093/esj/aakag023.1209), presented at the European Stroke Conference 2026 under the identifier ESOC2026YS125, reports that DMT inhibits spreading depolarisations (SDs) in brain slices prepared from sigma-1 receptor (S1R) knockout mice — and, critically, does so more effectively than in wild-type tissue. This is, to put it with characteristic British understatement, inconvenient for the prevailing narrative.
For some years now, the leading mechanistic story for DMT's putative neuroprotective effects in acute ischaemic stroke has centred on the sigma-1 receptor. The logic ran roughly thus: DMT is an endogenous agonist at S1R; S1R activation modulates calcium signalling, attenuates oxidative stress, and has demonstrated neuroprotective properties in various models; therefore DMT's capacity to limit ischaemic damage is most plausibly S1R-mediated. This was not an unreasonable chain of inference. It was, however, incomplete — and the Exeter data suggest it may have been pointing in the wrong direction entirely, or at the very least overstating the contribution of one receptor system at the expense of others.
Spreading depolarisations are massive, slow-moving waves of near-complete neuronal and glial depolarisation that propagate through injured cortex and are now understood to be a major secondary injury mechanism in stroke, traumatic brain injury, and subarachnoid haemorrhage. They are, if you like, the aftershocks following the initial earthquake — each one expanding the penumbral damage. An agent capable of suppressing SDs would have genuine translational significance. That DMT appears to do so is interesting. That it appears to do so more robustly in the absence of sigma-1 receptors is decidedly more than interesting; it is a mechanistic reorientation.
What this likely implicates
If the effect on SDs is not running through S1R, then the obvious candidates are the aminergic receptor pathways — serotonergic (5-HT2A, 5-HT2C, 5-HT1A) and possibly trace amine-associated receptors (TAAR1), all of which DMT engages with meaningful affinity. The enhanced efficacy in knockouts is particularly suggestive: it raises the possibility that S1R activation might actually be counteracting or buffering some of DMT's anti-SD effects through a parallel signalling pathway, such that removing it unmasks the full potency of the aminergic contribution. This would be a rather elegant pharmacological irony — the receptor everyone assumed was the hero turns out to be, at best, a bystander and, at worst, a mild antagonist of the desired effect.
One should, of course, be measured. This is a conference abstract reporting ex vivo brain slice data. We do not have access to the full dataset, the number of slices and animals used, the concentration–response characteristics, or the precise SD induction protocol. Brain slice electrophysiology is a robust technique for studying SDs, but it removes the preparation from systemic circulation and the immune response, both of which matter enormously in stroke. The leap from slice to clinic remains vast.
Translational consequences
Nevertheless, for those following the clinical pipeline — Algernon Pharmaceuticals' programme with DMT for stroke, and the broader interest in non-psychedelic DMT applications — this finding matters. If your regulatory strategy and dose-finding rationale are built on a sigma-1 receptor story, one would want to revisit pharmacodynamic biomarkers, animal model selection, and possibly dose optimisation logic. An aminergic mechanism would imply different structure–activity relationships for analogue development, different off-target risk profiles, and a different therapeutic window. It does not invalidate the programme. It complicates the map.
The Exeter group's involvement is worth noting. The university has been building a quiet but increasingly substantive body of work around DMT pharmacology and its intersection with cerebrovascular injury, and this latest contribution — provocative, cleanly framed, and presented at a major stroke conference rather than a psychedelics meeting — signals a seriousness of translational intent that one suspects will be rather more difficult to ignore going forward.
Also worth a glance
A systematic review and meta-analysis from Exeter- and Imperial-affiliated authors (DOI 10.1177/02698811261430518) pools DMT and 5-MeO-DMT studies for substance misuse outcomes and arrives at a large effect size (Hedges' g = 0.94), though the authors themselves flag an I² of 96.9% and high risk of bias across included studies — treat it as a useful cartography of the current evidence terrain rather than a verdict. Separately, a bioRxiv preprint (Preprint 42079221) examines serotonergic polypharmacology of 2-halogenated tryptamines, offering structure–activity data on halogen substitutions at the 2-position that will interest anyone working on DMT analogue design and receptor selectivity tuning.
Marginalia
One of the more underappreciated features of pharmacology as a discipline is that removing a target can teach you more than activating it ever did. The sigma-1 receptor knockout mouse was developed to prove the receptor's importance; it is a quiet comedy of science that it may end up demonstrating the opposite.